Transnasal endoscopes, also known as small-caliber, ultrathin or ultra-slim endoscopes, are very similar to standard or slim endoscopes except for their outer diameter, which is less than 6 mm, and their working channel, which is usually only 2 mm in diameter. Special biopsy forceps with a diameter of 1.8 mm are required for the working channel. (1)

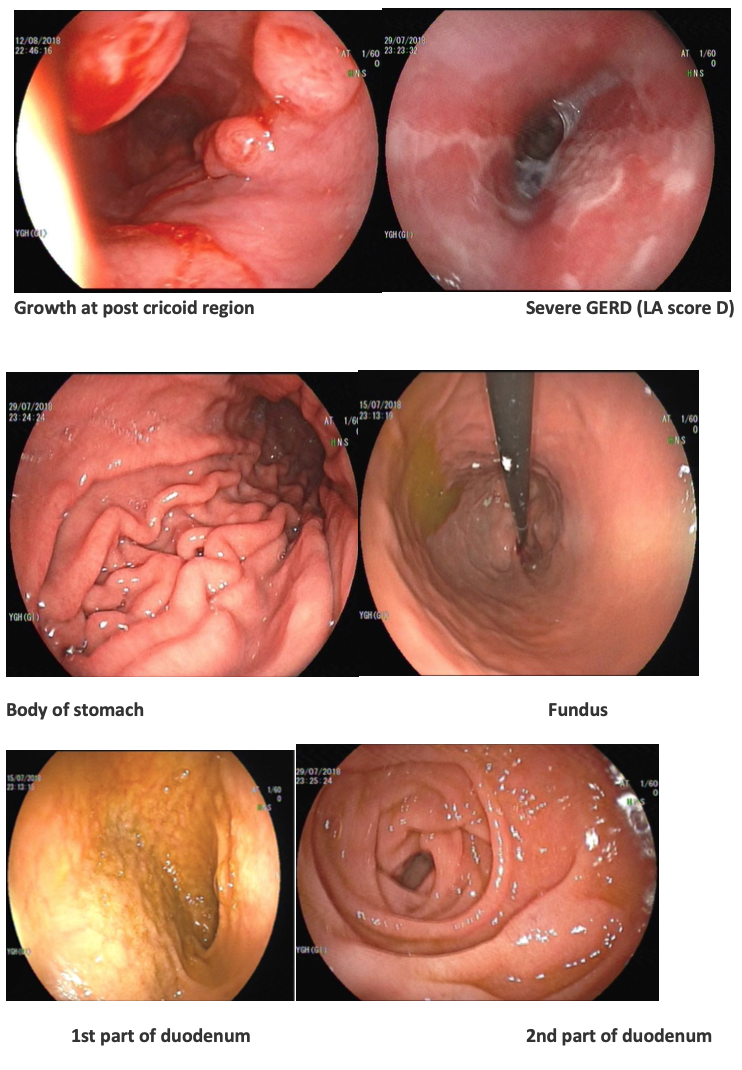
Transnasal endoscopy is available in civil government hospitals in Myanmar since 2015 and we can make diagnosis of the upper part of digestive system (oesophagus, stomach and duodenum).
Transnasal endoscopy is very similar test to a gastroscopy. In transnasal endoscopy a much smaller camera is introduced through the nose (not into the mouth like gastroscopy) down to the back of the throat and into the oesophagus. (2)
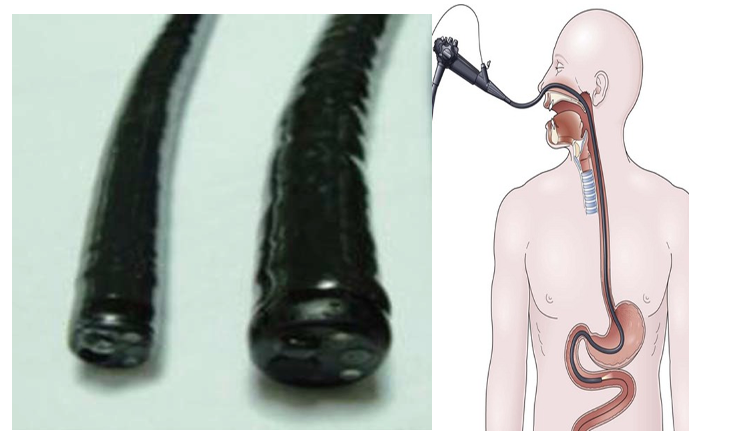
Relative diameters of an ultra-thin endoscope (left, 5.9 mm)
and a standard gastroscope (right, 8.8 mm)
Patients generally tolerate the procedure better as the camera does not touch the back of the tongue so they are unlikely to gag or retch during the procedure.The procedure is performed sat up and as the camera is not touching the back of the tongue patient can talk throughout the procedure. (2)
The test is often used to investigate the symptoms such as indigestion, heartburn, stomach pain, difficulty in swallowing or to exclude other abnormalities. Although the camera is thin, it is still big enough to allow biopsies to be taken to help with the diagnosis. (2)
The procedure takes 5 to 15 minutes and is commonly performed with local anesthetic only although sedation can be used if preferred. (2)
Advantages
More comfortable and tolerable than unsedated transoral endoscopy
Safer and cost-effective than sedated transoral endoscopy
Elimination of all side effects due to sedation
Total procedure time is shorter than sedated transoral endoscopy
No or minimal hemodynamic changes
No intravenous line is necessary routinely
Patient can speak, watch and discuss during procedure
No need for mouthpiece
Evaluation of nasal cavity, pharynx and larynx
Can be done in sitting position
Visual satisfaction for patients (1)
Limitations
Needs nasal pretreatment
Nasal pain and discomfort
Mild epistaxis
Limited functionality (suction, air, water)
Extreme flexibility of scope body
Narrow working channel. Not appropriate for through the scope interventional procedures
Needs extra training
No HD image capabilities
Higher insertion failure rate
Longer examination time
Not appropriate for patients with nasal problems (1)
Transnasal endoscopy is feasible, effective and well tolerated for screening of esophageal and gastric varices in patients with chronic liver disease. It can be performed in outpatient clinics safely and without the use of sedation. (3)
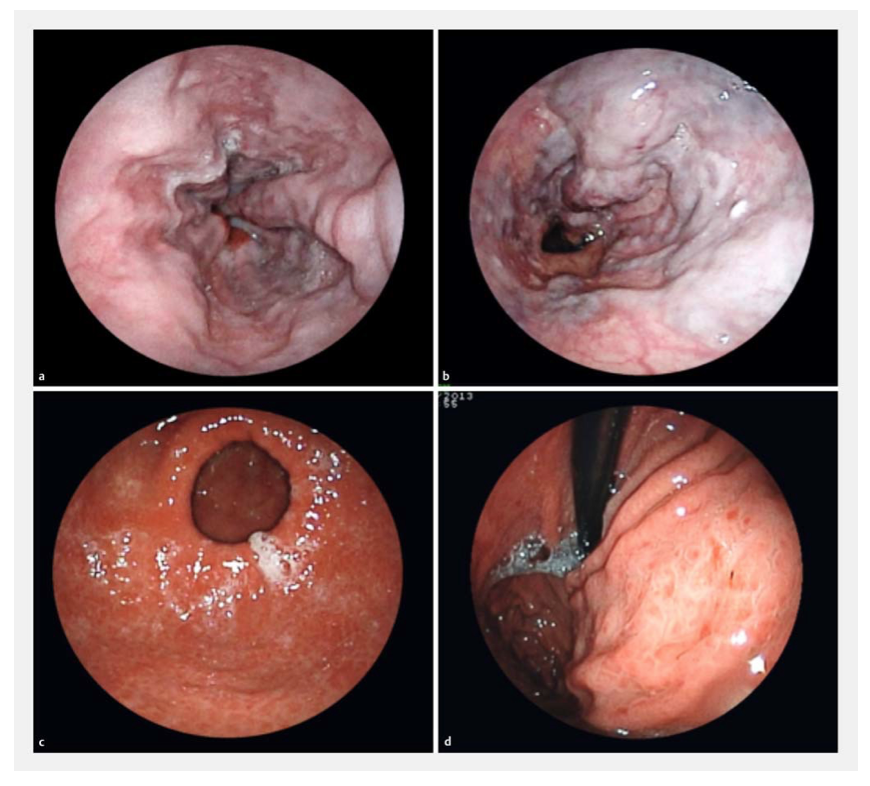
Endoscopic findings related to portal hypertension. a Esophageal varices of small and medium caliber. b Large-caliber esophageal varices with red spots. c, d Hypertensive gastropathy. (3)
Ideally, TNE should be considered in asymptomatic patients desiring screening for BE based on family history or other factors. TNE might also be appropriate for patients with symptoms strongly suggestive of esophageal pathology in whom standard endoscopy is problematic or unappealing or in whom a complete EGD is not warranted. It will be interesting to see if the coming years see TNE without sedation enter mainstream practice and widespread use. (4)
In recent years, using the advantage of their thin diameter, transnasal endoscopes has been used for different endoscopic therapeutic applications, including nasojejunal feeding tube insertion, percutaneous gastrostomy and jejunostomy, direct cholangio scopy with biopsy and lithotripsy, and a double scope technique for some endoscopic interventions. The thin diameter of these scopes is an important advantage to pass through gastrointestinal strictures where standard scopes have failed. (1)
References
( 1 ) World J GastrointestEndosc2014, February 16; 6(2): 41-48
( 2 ) www.leedsth.nhs.uk › Services › Endoscopy › About your procedure
( 3 ) de Faria, A. A., Dias, C. A. F.,Moetzsohn, L.D., de Castro Carvalho, S., Ferrari, T. A., &Arantesl, V. N. (2017) Feasibility of transnasal endoscopy in screening for esophageal
and gastric varices in patients with chronic liver disease.Endoscopy International Open; 05: E646–E651.
(4) Adler D.G.Gastrointestinal Endoscopy 2012, Volume 75, No. 5
- Professor and Head, Department of Gastroenterology, Yangon General Hospital
- Professor, Department of Gastroenterology, Yangon General Hospital
- Associate Professor, Department of Gastroenterology, Yangon General Hospital
- Consultant Gastroenterologist, Department of Gastroenterology, Yangon General Hospital
- Doctorate student, Department of Gastroenterology, University of Medicine 1, Yangon
Thein Myint1, Moe Myint Aung2, Tin Moe Wai3, Swe Mon Mya4, Mya Thet Nwe4, Sandar Win4, Thida Soe4, Su Su Hlaing5
Department of Gastroenterology, Yangon General Hospital