Summary
Spontaneous rupture of an ovarian artery aneurysm is a rare but usually life-threatening event. There have been only 26 cases reported in the English literature. The majority of the cases were related to pregnancy and occurred during the peripartum or postpartum period. The diagnosis could have been missed but for the meticulous and timely interventions which avoided a catastrophic outcome.This is a case of a multiparous woman with rupture of a right ovarian artery aneurysm, causing massive retroperitoneal hemorrhage and hematoma that required surgical evacuation. Spontaneous rupture of the ovarian artery should be considered as one of the differential diagnosis in the immediate postpartum period especially when the clinical symptoms do not correlate with the amount of blood loss. A high index of suspicion, prompt diagnosis and intervention were the elements of a successful outcome in this case.
Background
Ruptured ovarian artery aneurysms are extremely rare life threatening condition. The first case was described in 1963.1 There have been 26 cases reported in the English literature.26 Majority of the cases were related to pregnancy and occurred during the peripartum or postpartum period.4,9,11,12 An association with uterine fibroids has also been noted 16 and there have been recent reports that were not directly associated with pregnancy.26 Ruptured ovarian artery aneurysm usually mimics other less life-threatening conditions in its clinical presentation. This can result in delay diagnosis and treatment that may have catastrophic outcomes. Hence, early diagnosis and prompt treatment is required for the maximum chance of survival of mother and child.25 This was a case of ruptured ovarian artery aneurysm which was managed successfully by exploratory laparotomy at resources limited small hospital, Myanmar.
Case Presentation
A 37 year-old female, Para 7+0 was presented to on-call surgeon for unexplained shock on first day of uneventful normal vaginal delivery. Before occurring of fainting attack, she had complained of dizziness, sweating and abdominal distention without any remarkable abdominal pain. She had no remarkable amount of bleeding per vagina during postpartum period.
She had no fever, nausea, vomiting, diarrhea, or cough. She had no history of abdominal trauma, and her past medical and family history were not significant. She did not have hypertension or cardiovascular disease and had not taken any anticoagulants.
On examination, she was distressed and anemic. Her pulse rate was 132/min, blood pressure, 60/40 mmHg, body temperature, 37°C and blood oxygen saturation 98% respectively. Her hemoglobin level was 7.7gm%. Her coagulation profile and blood sugar were within normal limits.
On physical examination, her abdomen was distended, but no remarkable tenderness and muscle guarding. Bowel sounds are absent. A pelvic examination revealed no bleeding per vagina. After fluid resuscitation, her blood pressure became 70 / 60 and pulse rate was 120/ min. Although 2 units of fresh whole blood was issued, she was still hypotensive and anemic. Urgent abdominal ultrasonography demonstrated a large hypoechoic (10 x 12cm) mass in right side of abdomen with free fluid within the peritoneal cavity. The Sonographer’s remark was possible ruptured ovarian cyst or retroperitoneal tumor. Computed Tomography was unavailable in this small hospital.
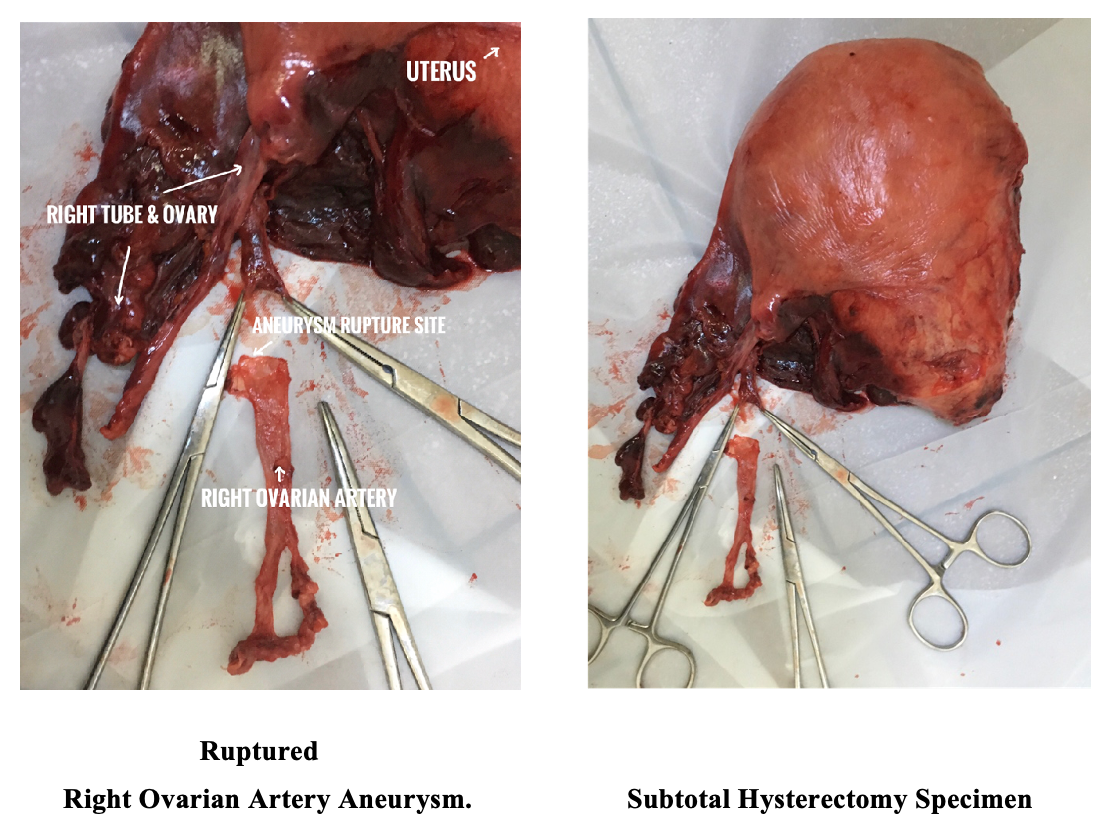
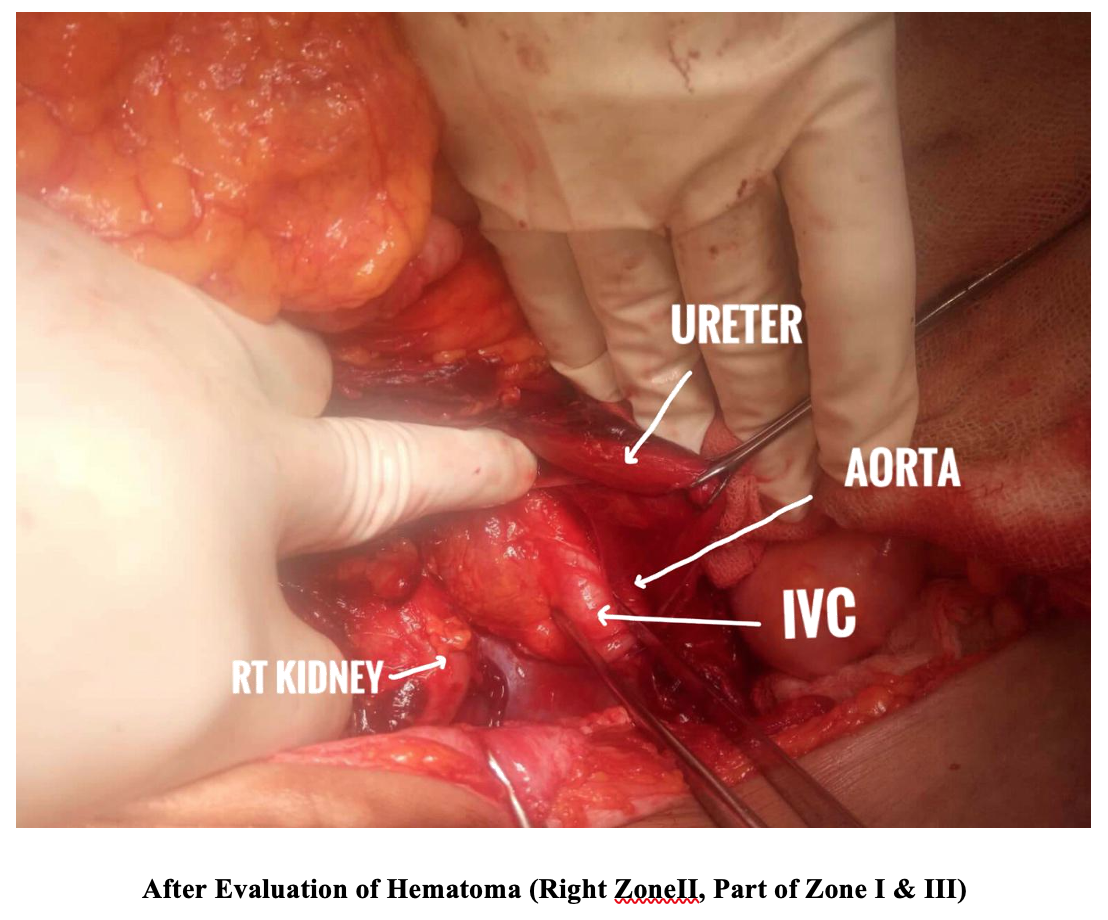
Based on this ultrasonography results and the clinical presentation, we decided to perform an emergency laparotomy. The laparotomy revealed intraperioneal hemorrhage( about 0.5 liter) apparently caused by intra-abdominal extension of retroperitoneal hemorrhage. The small and large intestines were dilated from a paralytic ileus. The massive expanding retroperitoneal hematoma involving the whole Right Zone II, part of Zone I and Zone III was found. When the right colon and the intestinal mesentery were rotated medially, a massive retroperitoneal hematoma approximately 2000 grams were exposed and then removed. These procedures exposed the right ovarian artery which was found to be skewed, dilated and ruptured. The ruptured right ovarian artery was ligated and resected just beyond Aorta proximally and near right ovary distally. Examination of the right retroperitoneal space revealed no other abnormality or injury. Both Fallopian tubes and ovaries were normal. Subtotal Hysterectomy was also done because of an atonic uterus and risk of postpartum hemorrhage. Postoperative course was unremarkable, and the patient was discharged from the hospital on the 8th postoperative day.
The segment of the ovarian artery removed at laparotomy was approximately 8 cm long, and part of the segment was dilated and tortuous. Microscopic examination showed thick-wall blood vessels lined by single layer of flattened endothelium with marked muscular hyperplasia of tunica media and foci of hemorrhages within tunica media. Pathological diagnosis was compatible with fibromuscular hyperplasia, tunica media of right ovarian artery.
Discussion
Ovarian aneurysmal rupture is a rare life threatening emergency condition. This rare condition can result in catastrophic hemorrhage, serious morbidity, and even death without prompt diagnosis and immediate intervention. There is a high index of suspicion in women during pregnancy, peripartum and postpartum period whose blood loss is not commensurate with their clinical scenarios and this should prompt early imaging studies for diagnosis and urgent treatment.
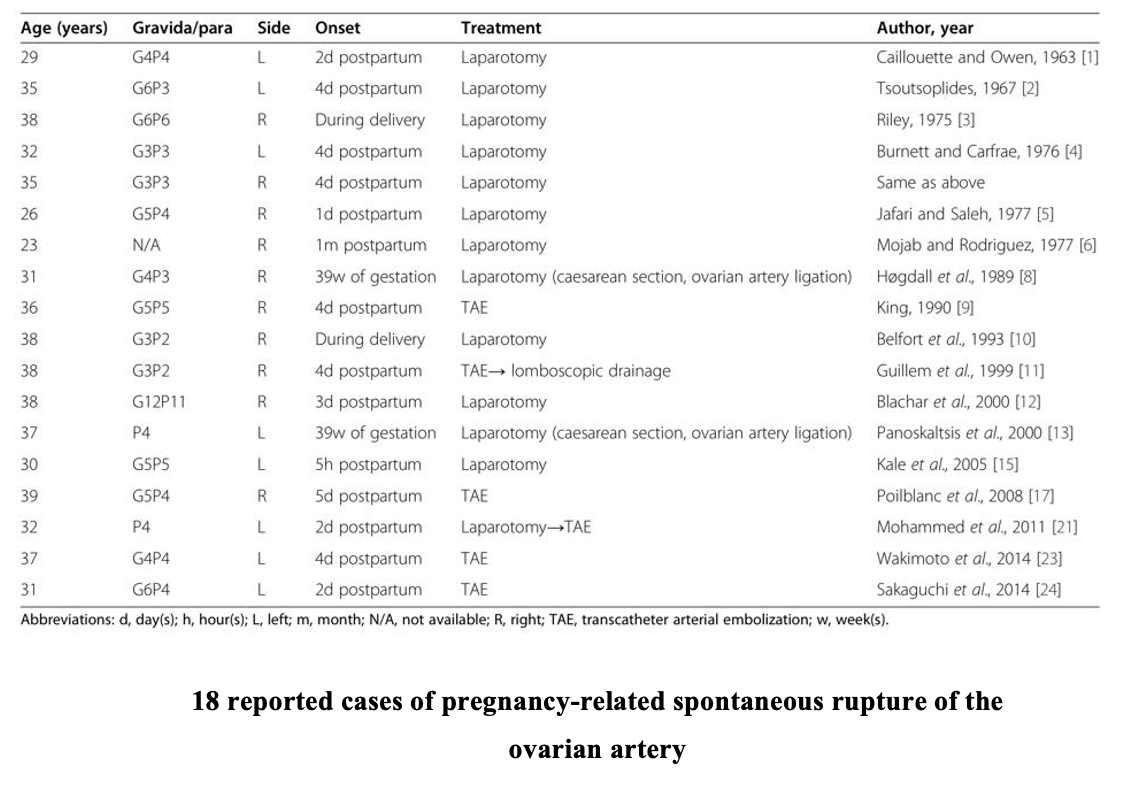
Various hemodynamic and hormonal factors have been suggested for the pathogenesis.4,9,12 Because a ruptured ovarian artery aneurysm mostly occurs in women of high parity, the repeated hemodynamic and endocrine changes during pregnancy are thought to be the cause of arterial alterations that may lead to new aneurysm formation and or weakening of pre-existing aneurysms.4,25 In addition to the physiologic changes of pregnancy, hypertension might be a risk factor for rupture of ovarian artery aneurysm.18
Majority of previously reported ovarian artery aneurysms usually present with spontaneous rupture in the puerperium 1,4,11, especially in the immediate postpartum periods. 9 It has also been reported in non pregnant patients 18 and sometimes during the antepartum period.8 Very few asymptomatic cases are incidentally identified during evaluation for other reasons.27 The most common presentation of ruptured ovarian artery aneurysm is the acute flank pain or abdominal pain.9,12
In earlier reported cases, the diagnosis was always obtained by exploratory laparotomy. Ultrasonography is a safe and rapid method of detection of intraperitoneal effusion.11 Computed tomography or magnetic resonance imaging can then be used to search for the underlying cause, which is usually an intraperitoneal hematoma.11,16 In our case, intraperitoneal hematoma was first shown by ultrasonography, diagnosis was confirmed during laparotomy. Laparotomy is a reliable emergency treatment for spontaneous or traumatic retroperitoneal hemorrhage. 28 Ruptured ovarian artery aneurysm may be surgically treated by adnexectomy or ligation proximal and distal to the rupture.12,25 A minimally invasive procedure, TAE is currently considered to be the treatment of choice. 26 Because most patients with ovarian artery aneurysm are asymptomatic and rupture is an uncommon event, this condition may be underdiagnosed and the risk factors for rupture have not yet been studied in depth. Additional case reports may help clarify the nature of ovarian artery aneurysms.2
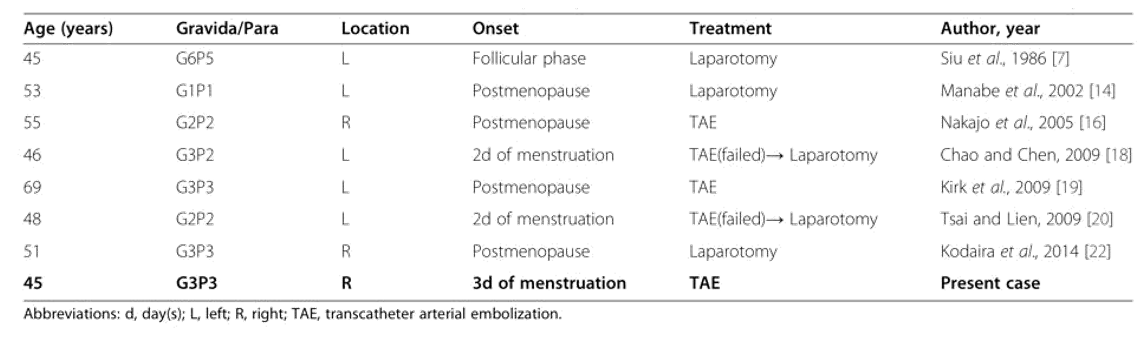
7 reported cases of pregnancy-unrelated spontaneous rupture of the ovarian artery
Conclusion
Although rupture of an ovarian artery aneurysm is extremely rare, it is life-threatening and is often associated with a non-specific clinical picture. Awareness of this entity and a high index of suspicion may lead to early diagnosis and treatment.
Take home message
Spontaneous rupture of the ovarian artery should be considered as one of the differential diagnosis in the immediate postpartum period especially when the clinical symptoms do not correlate with the amount of blood loss. A high index of suspicion, prompt diagnosis and intervention can save the patient’s life.
References
- Caillouette JC, Owen HW: Postpartum spontaneous rupture of an ovarian-artery aneurysm. ObstetGynecol 1963; 21: 510―511.
- Tsoutsoplides GC. Post-partum spontaneous rupture of a branch of the ovarian artery. Scott Med J. 1967;12:289–90.
- Riley PM. Letter: Rupture of right ovarian artery aneurysm during delivery. S Afr Med J. 1975;49:729.
- Burnett RA, Carfrae DC. Spontaneous rupture of ovarian artery aneurysm in the puerperium. Two case reports and a review of the literature. Br J ObstetGynaecol. 1976;83:744–50.
- Jafari K, Saleh I. Postpartum spontaneous rupture of ovarian artery aneurysm. Obstet Gynecol. 1977;49:493–5.
- Mojab K, Rodriguez J. Postpartum ovarian artery rupture with retroperitoneal hemorrhage. AJR Am J Roentgenol. 1977;128:695–6.
- Siu KF, Luk SL, Kung TM. Spontaneous rupture of the ovarian artery. J R CollSurgEdinb. 1986;31:237–40.
- Høgdall CK, Pedersen SJ, Ovlisen BO, Helgestrand UJ. Spontaneous rupture of an ovarian-artery aneurysm in the third trimester of pregnancy. ActaObstetGynecol Scand. 1989;68:651–2.
- King WL. Ruptured ovarian artery aneurysm: a case report. J Vasc Surg. 1990;12:190–3.
- Belfort MA, Simon T, Kirshon B, Howell JF. Ruptured ovarian artery aneurysm complicating a term vaginal delivery. South Med J. 1993;86:1073–4.
- Guillem P, Bondue X, Chambon JP, Lemaitre L, Bounoua F. Spontaneous retroperitoneal hematoma from rupture of an aneurysm of the ovarian artery following delivery. Ann Vasc Surg. 1999;13:445–8.
- Blachar A, Bloom AI, Golan G, Venturero M, Bar-Ziv J. Case reports. Spiral CT imaging of a ruptured post-partum ovarian artery aneurysm. ClinRadiol. 2000;55:718–20.
- Panoskaltsis T, Padwick M, Thomas JM, el Sayed T. Spontaneous rupture of ovarian arterial aneurysm in the antenatal period. ActaObstetGynecol Scand. 2000;79:718–9.
- Manabe Y, Yoshioka K, Yanada J. Spontaneous rupture of a dissection of the left ovarian artery. J Med Invest. 2002;49:182–5.
- Kale A, Akdeniz N, Erdemoglu M, Ozcan Y, Yalinkaya A. Spontaneous rupture of the ovarian artery following spontaneous vaginal birth. Saudi Med J. 2005;26:1826–7.
- Nakajo M, Ohkubo K, Fukukura Y, Nandate T. Embolization of spontaneous rupture of an aneurysm of the ovarian artery supplying the uterus with fibroids. ActaRadiol. 2005;46:887–90.
- Poilblanc M, Winer N, Bouvier A, Gillard P, Boussion F, Aubé C, et al. Rupture of an aneurysm of the ovarian artery following delivery and endovascular treatment. Am J Obstet Gynecol. 2008;199:e7–8.
- Chao L-W, Chen C-H. Spontaneous rupture of an ovarian artery aneurysm: case report and review of the literature. GynecolObstet Invest. 2009;68:104–7.
- Kirk JS, Deitch JS, Robinson HR, Haveson SP. Staged endovascular treatment of bilateral ruptured and intact ovarian artery aneurysms in a postmenopausal woman. J Vasc Surg. 2009;49:208–10.
- Tsai M-T, Lien W-C. Spontaneous rupture of an ovarian artery aneurysm. Am J Obstet Gynecol. 2009;200:e7–9.
- Mohammed N, Rai H, Koo B, Hoveyda F. Postpartum rupture of ovarian artery. J ObstetGynaecol. 2011;31:548–9.
- Kodaira Y, Iwamura T, Hoshino H, Takahashi K, Kawahigashi Y, Matsumoto K. Spontaneous rupture of aneurysms of the ovarian artery at times remote from pregnancy. J Nippon Med Sch. 2014;81:101–5.
- Wakimoto S, Hidaka N, Fukushima K, Kato K. Spontaneous post-partum rupture of an ovarian artery aneurysm: A case report of successful embolization and a review of the published work. J ObstetGynaecol Res. 2014. doi:10.1111/jog.12535
- Sakaguchi I, Ohba T, Ikeda O, Yamashita Y, Katabuchi H. Embolization for post-partum rupture of ovarian artery aneurysm: Case report and review. J ObstetGynaecol Res. 2014. doi:10.1111/jog.12561
- Barrett JM, Van Hooydonk JE, Boehm FH. Pregnancy-related rupture of arterial aneurysms. ObstetGynaecolSurv. 1982;37(9):557-66.
- Toyoshima M, Kudo T, Igeta S, et al. Spontaneous retroperitoneal hemorrhage caused by rupture of an ovarian artery aneurysm: a case report and review of the literature. J Med Case Rep. 2015;9:84. Published 2015 Apr 18. doi:10.1186/s13256-015-0553-4
- Slaba S, Kazzi H, Abd O, Nassar J, Nasnas R. Glue embolization of an unruptured ovarian aneurysm. J Mal Vasc. 2010;35(4):266-9.
- Mattox KL, Burch JM, Richardson R, Martin RR: Retroperioneal vascular injury. SurgClin Nor Am 1990; 70: 635―653.
Kyaw Min Tun1, MyintZu Phone2,Zaw Min Tun3, Nay Nwe Shwe4, HninEi Hlaing5, Saw Aung Aung5,
1 SAS Surgeon, Kawkareik District Hospital, 2 SAS Obstetrics & Gynecologist, Kawkareik District Hospital, 3 Consultant Anesthesiologist, Kawkareik District Hospital, 4 Consultant Radiologist, Kawkareik District Hospital, 5 Assistant Surgeon, Kawkareik District Hospital