Introduction:
In management of hypertension especially in young people, we should look for underlying cause because most of these cases are secondary to underlying conditions. Another important point not to forget are associated risk factors and target organ damage.
Some of the causes like Cushing’s syndrome, Acromegaly, Renal Artery Stenosis and Coarctation of Aorta can be diagnosed relatively easy by proper history taking and thorough physical examination. But in the case of “Phaeochromocytoma”, because of the nature of the disease’s history (paroxysmal episode) and no solid physical signs, the diagnosis may usually be late and even labeled the patients as “Psychogenic” in some instances.
Diagnosis and management of hypertension due to Phaeochromocytoma” is not only straightforward, but also need MDT (Multidisciplinary Team) approach .In this issue of MJCMP with the Theme of “Hypertension”, we want to share our case for the benefit of the readers and young generation.
Case summary:
Last 12 years ago, a 46 year old Myanmar Lady Consulted a Physician for non specific symptoms like occasional mild headache, stiffness and tiredness. History, examination and basic investigations revealed mild hypertension with type II Diabetes Mellitus, hyperlipidaemia without any target organ damage. Life style modification together with Oral Hypoglycemic drugs( Gliclazide MR and Metformin) ,ACE inhibitor (Perindropil) , Statin were started and all problems were fairly controlled for (7) years after that her BP and blood glucose level were difficult to control and need to increase dose, add another antihypertensive agent amlodipine. On detailed and proper review of her history, she recalled very occasional episodes of experiencing sudden onset of palpitation, chest discomfort and headache, but she thought these symptoms were attributable by her family and domestic stressful conditions. Because of poor control , she was closely followed up and at one clinic visit , she was found to have quite high BP and high random blood sugar and sweating and it resolved after (30) minutes rest in clinic . She also gave history of fainting attacks 2-3 times in a week on standing from sitting position, but there was no significant postural drop of BP at clinic.
On one day in September 2016, she was admitted to hospital as emergency because she has a head injury after a fall due to fainting inside bathroom. After exclusion of intracranial and cranial pathology by neuro imaging, her lacerated wound was stitched and necessary and appropriate management of her current and pre-morbid conditions were given. Since blood glucose level was very high, Insulin therapy was added to oral medications .She was safely discharged after a week and advised to continue treatment including Insulin but she was readmitted after a few days with hypoglycemia and then again with severe hyperglycemia and high glucose . Her symptoms like palpitation, headache, sweating became more frequent at home although these were not detected at clinic or hospital.
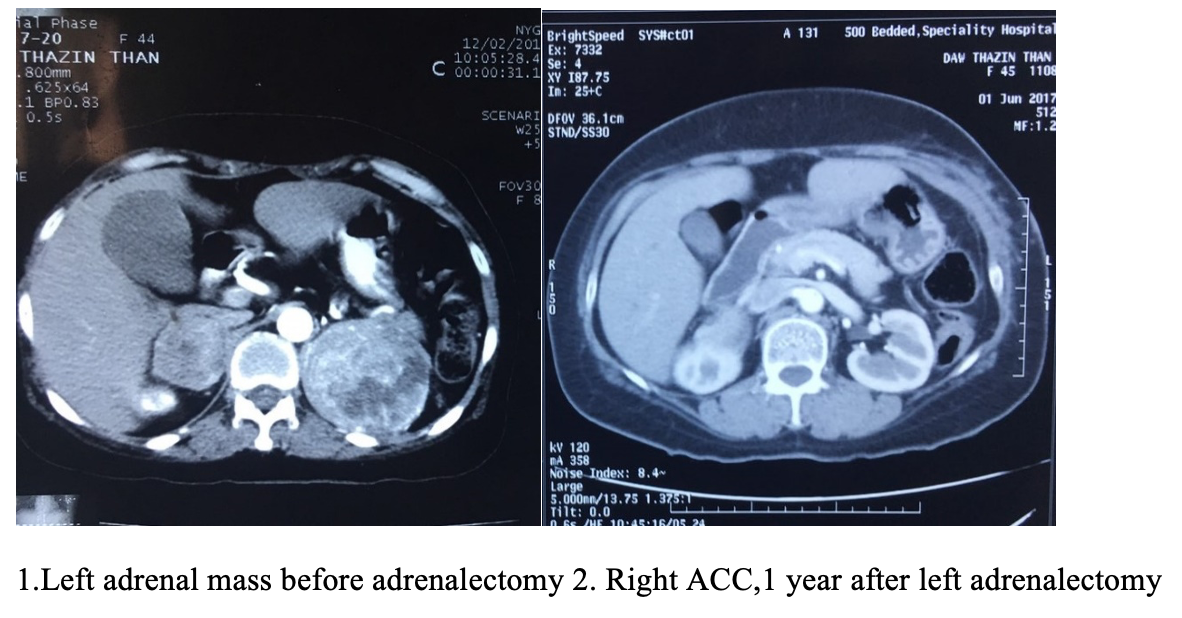
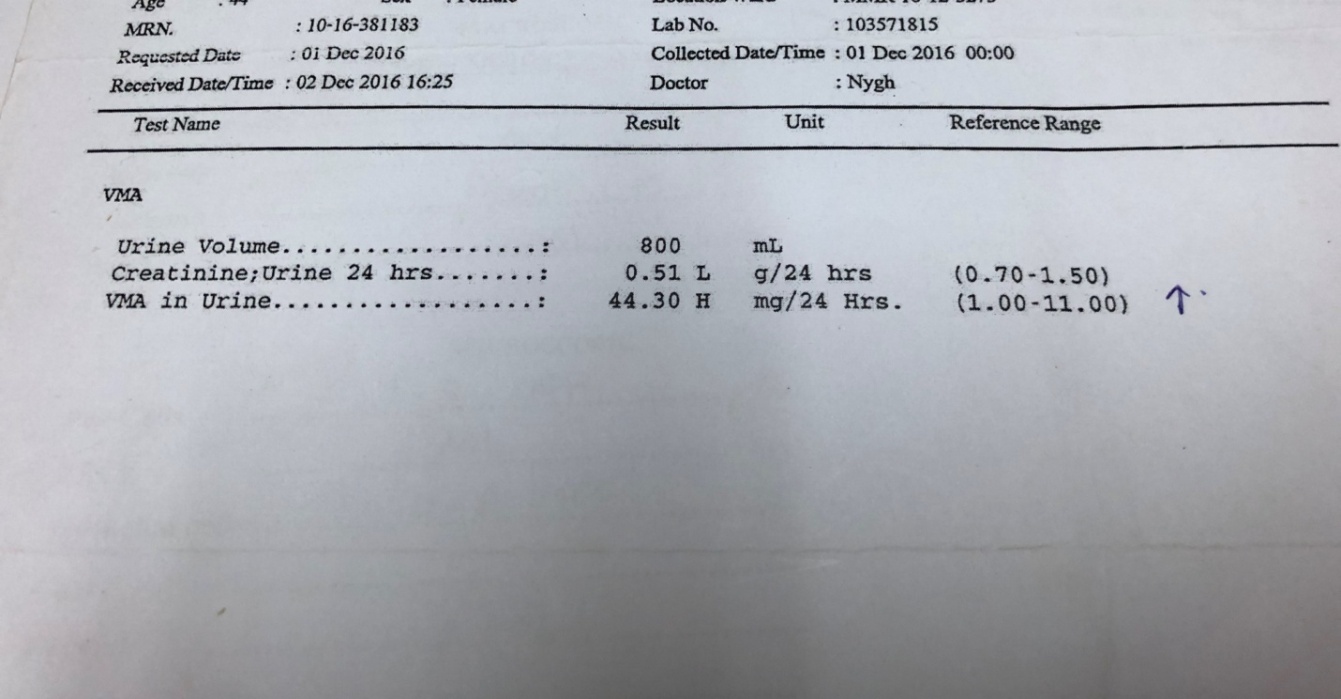
Therefore, the possibility of “Phaeochromocytoma” as a cause of paroxysmal episodes of such symptoms with postural hypotension and difficult to control BP and blood glucose was considered and further necessary investigations including special imaging were organized. For measuring urinary VMA, the standard protocol was followed by switching ACEI with doxazosin, for 2 weeks and 24 hour Urinary VMA was significantly high ( 44.3 mg/24 hours). She was found to have bilateral enlargement of both adrenal glands (left > right), not so obvious in ordinary abdomen ultrasonography, but only with 200 sliced CT imaging and MRI. After that, the treatment was modified, control BP with Labetalol and Control glucose with Insulin therapy and she was consulted with Urosurgeon for necessary intervention.
She was admitted to Urosurgical Department of 500 bedded Yangon Specialty Hospital on 1st March 2017. After meticulous screening and assessment by Physicians, Surgeons and Anesthetists, left adrenalectomy was performed on 3rd April 2017. Operation time lasted for one and half hours and as expected in surgery of such adrenal tumour, there was a stormy course intra and postoperative period (like rapid surge of BP after opening and handling adrenal gland and tremendous fall of BP after removal of adrenal tumour and so on) which was efficiently handled by the Team work especially Anesthetists and endocrinologists. BP and glucose control seemed to be better after left adrenalectomy with very occasional paroxysmal attacks. She was consulted with Endocrinologist from Department of Endocrinology , YGH since before left adrenalectomy and Medical Oncologist was also involved since after first operation .After first operation , her post operative cortisol levels are well maintained above >294 nmol/L so that she didn’t need steroid replacement after surgery.
Another shocking news occurred after Thingyan Holiday when the biopsy report by the Histopathologist came back as “Adrenocortical Carcinoma”. Since the patient’s symptoms were in favor of excess adrenal medullary hormones rather than adrenal cortical hormones, second opinion for the biopsy was sought from a famous pathologist and given the report back as “Phaeochromocytoma” with a differential diagnosis of Adrenocortical Carcinoma”, suggesting to proceed IHC (immune histochemical stain with Chromogranin) and or Synaptophysin for Phaeochromocytoma and Vimentin for adrenocortical carcinoma. With the use of IHC, the tumor was found to be Vimentin negative, Synaptophysin positive so the diagnosis of Phaeochromocytoma was confirmed.
Since bilateral adrenal tumors have tendency to be potentially malignant, the case was discussed among multiple disciplines and finally decided to remove the right adrenal gland as well .She was admitted again to Urosurgical Ward of 500 bedded YSH on 24th July 2017. After full preop assessment and preparation, right adrenalectomy with removal of parahilar lymph nodes was performed on 10th August 2017. Histology of removed right adrenal tumour showed similar appearance to previous left adrenal tumor.
After recovery from extensive surgery, she was seen by Medical Oncologist for management of her bilateral adrenal tumours and started cycles of chemotherapy to be completed. Since both adrenals are removed totally , there was definitely lack of hormones produced by all layers of adrenals (aldosterone, cortisol and catecolamines) and among them , aldosterone and cortisol are produced mainly by adrenals so that Endocrinologist has to monitor her closely. She developed cortisol deficiency symptoms clinically as well as biochemically after surgery (cortisol level after 2nd operation 3.11nmol/L) so that she was given replacement of adrenal corticoid hormones appropriately.
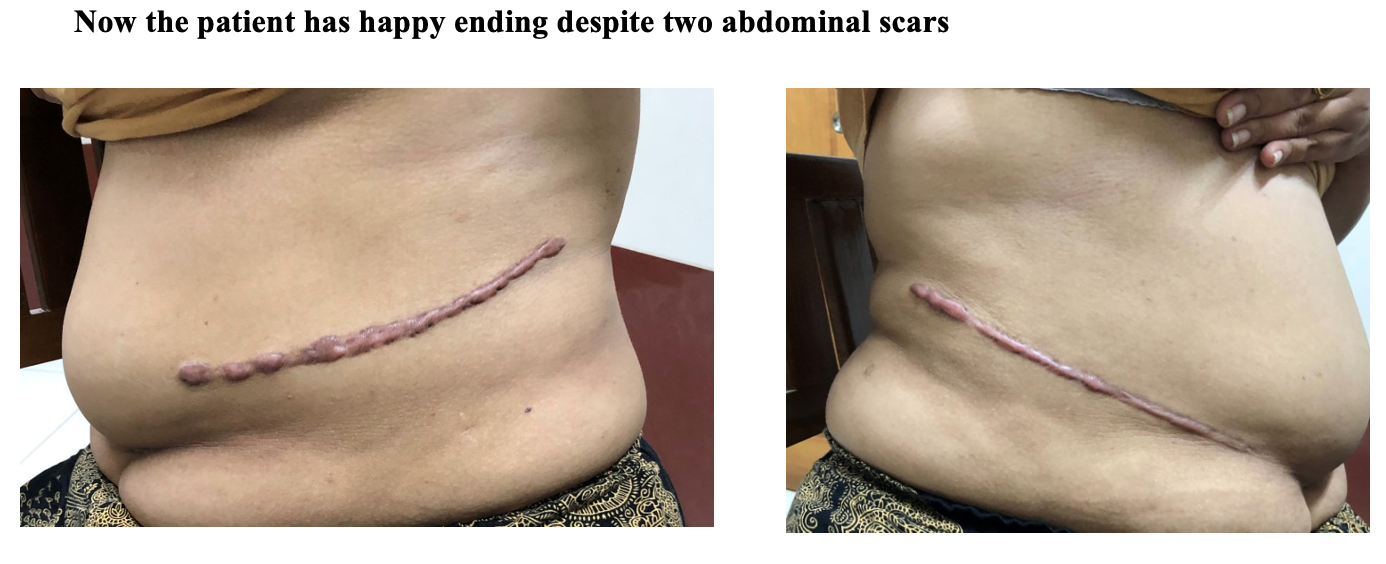
She is now under continuous care by her primary physician, endocrinologist and oncologist and generally stable and currently on the following medications: Hydrocortisone 10mg:5mg:5mg, Fludrocortisone 100mg OD, Metformin 500 mg BD, Atorvastatin 10 mg HS and clearly hypertension was well controlled without needing antihypertensive drugs.
The happy ending of the story is hypertension was totally cured and there is no recurrence of adrenal tumor after 2 years follow up CT scan.
Recheck investigations revealed: November 2018 (15 months post operation)
Creatinine 78 , Urea 7.6 , K 3.8, Na 133, uric acid 6.4 ,HbA1C 6.9 , USG – normal scan, Message for the readers: Young hypertension cases are not so uncommon. Most of these cases have underlying pathology and need to look for it. Among the underlying causes, Phaeochromocytoma is quite unique in misleading the attending clinicians due to its characteristics of paroxysmal nature and often lead to late discovery of the lesion. This case showed the value and beauty of Multidisciplinary Team approach in management consists of Primary Physician, Urosurgeons , Anaesthetists, Radiologists, Pathologists , Endocrinologists, Oncologists and all other Nursing Staff and Technicians whose combined effort saved the life of patient to have a good quality of life .
CT scan pictures
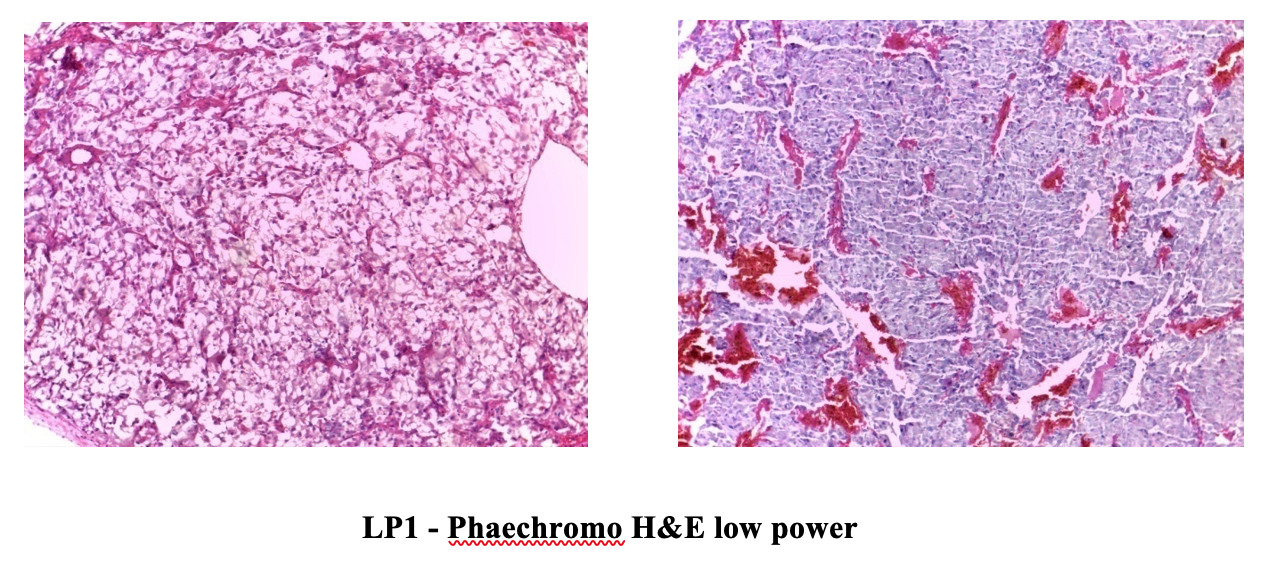
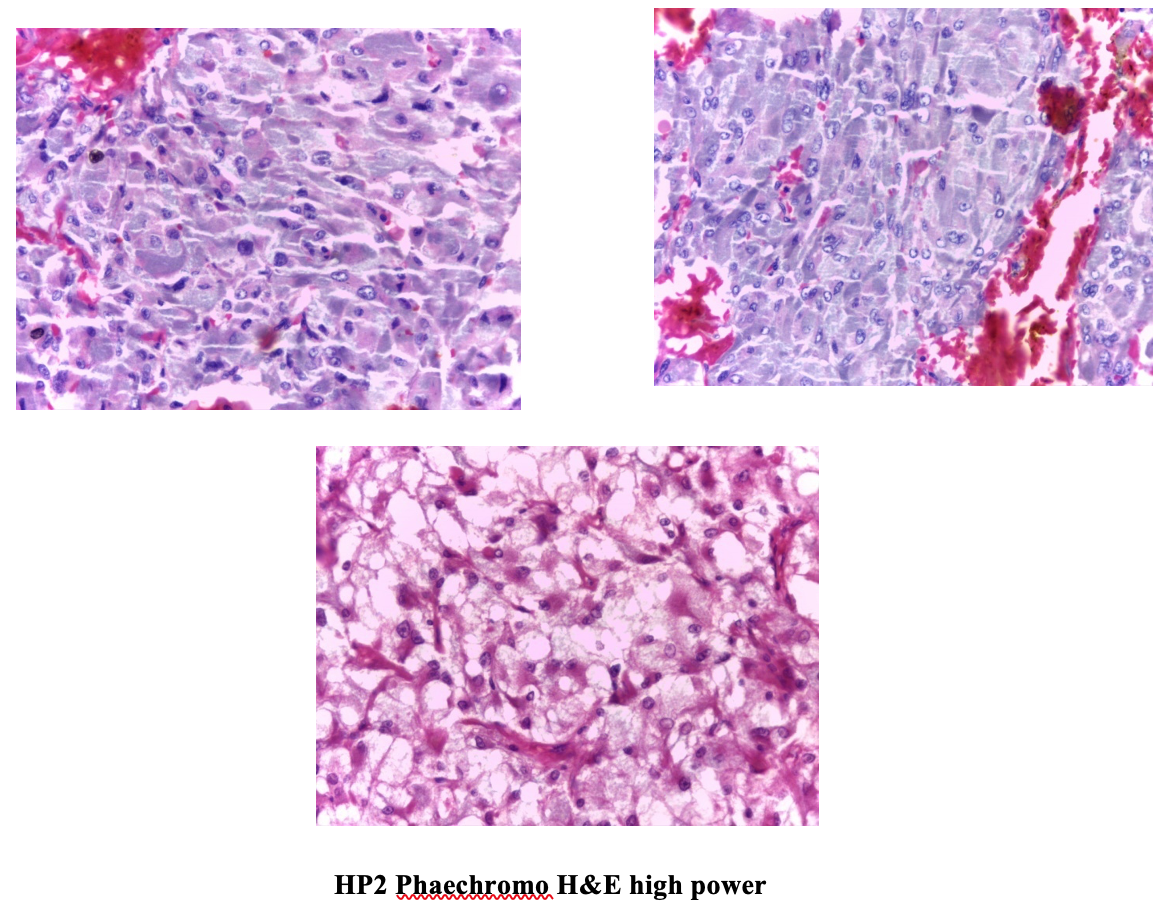
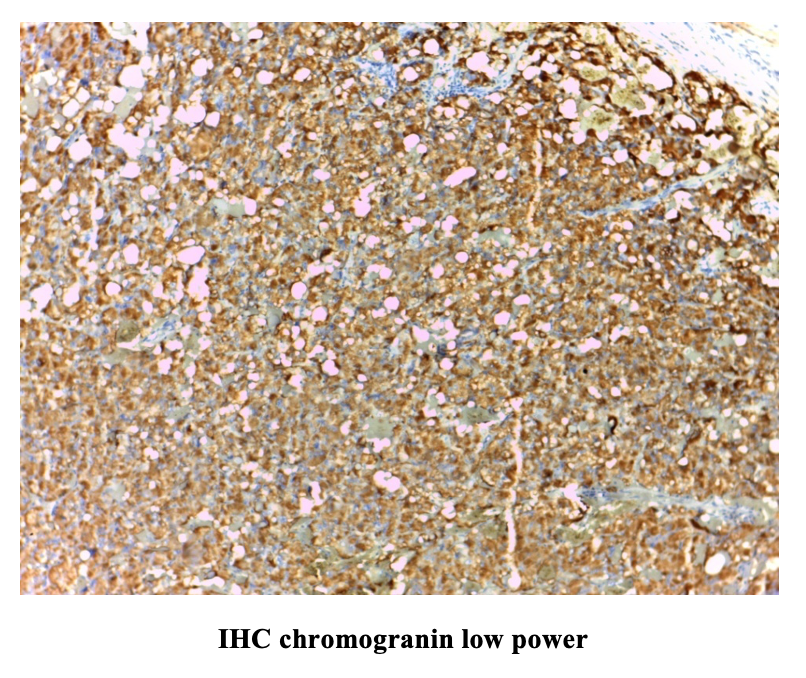
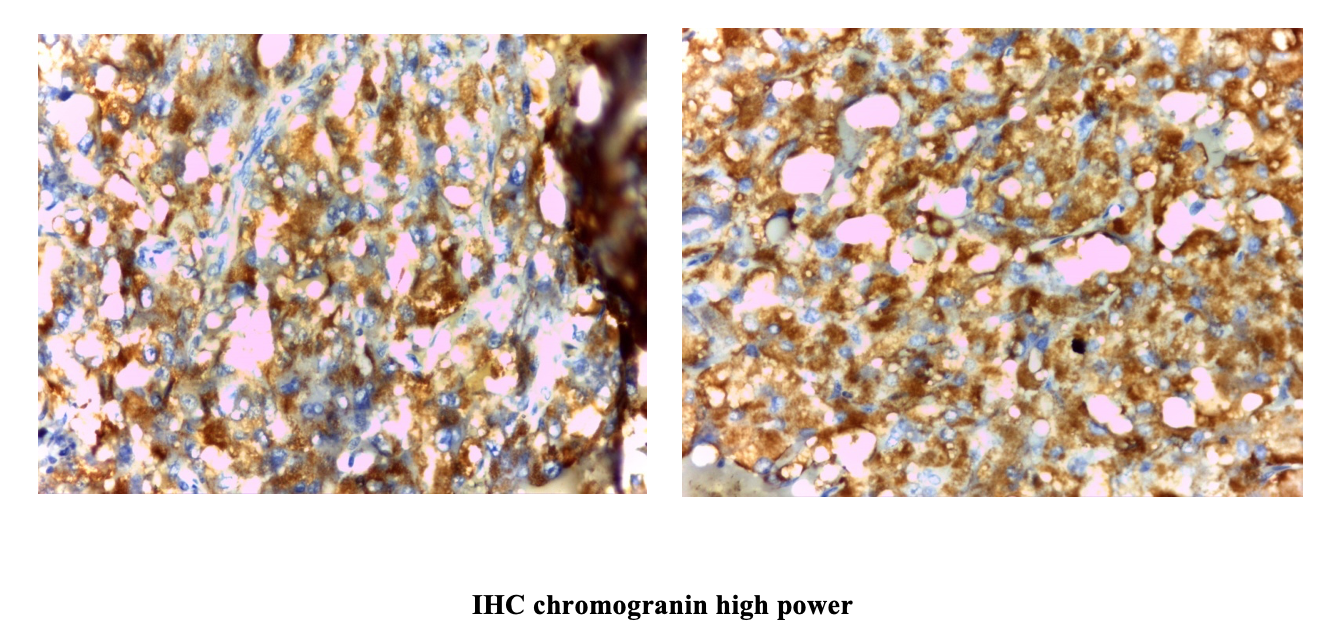
IHC Result: Vimentin negative, Synaptophysin positive . Therefore Final Diagnosis is Phaechromocytoma
Further Reading:
- Young Jr,W. F., et al. (2017) Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement, Endocrine Reviews,38(2). pp. 103-122. doi: 10.1210/er.2017-00054.
- Plouin PF, Duclos JM, Menard J, Comoy E, Bohuon C &Alexandre JM. Biochemical tests for the diagnosis of pheochromocytoma: urinary versus plasma determinations. BMJ 1981,282,853-854
- Werbel SS, Ober KP. Pheochromocytoma: update on diagnosis, localization, and management. Med Clin NorthAm. 1995;79:131-153.
- Yang, J., Shen, J. and Fuller, P. J. (2017) Diagnosing endocrine hypertension : a practical approach: Review Article, Asian Pacific Society of Nephrology. 22. pp. 663 – 677. doi: 10.1111/nep.13078.
Professor Nyunt Thein, Emeritus Professor, Former Head of Department of Medicine, University of Medicine (1) Yangon
Professor Khin Saw Than, Head of Department of Endocrinology, YGH
Professor Moe Wint Aung, Department of Endocrinology, YGH
Professor Kyaw Swar Hlaing, Former Head of Department of Urosurgery, YSH
Professor Kyaw Soe Kyaw, Head of Department of Urosurgery, NPT
Professor Aye Aye Myint, Former Head of Department of Pathology, University of Medicine (1) Yangon
Associate Professor Wai Wai Lwin, Department of Medical Oncology, YGH
Associate Professor Myo Thet Tin, Department of Pathology, YSH
Associate Professor Saw Aung Phyo Aye, Department of Radiology, YSH
Associate Professor Maung Maung Swe, Department of Anesthesiology, YSH