
The facial nerve is a mixed nerve providing both sensory afferent and motor efferent fibers that arises from pons. It passes laterally at the cerebello-pontine angle, and travels through the internal auditory canal. The nerve exits the stylomastoid foramen dividing into five branches to innervate the muscles of facial expression.
Visceral motor fibers of facial nerve innervate the lacrimal gland, stimulating reflex tearing of the ipsilateral eye. The somatic motor fibers supply all three parts of the orbicularis oculi muscle (palpebral, orbital, and lacrimal) that functions to close the ipsilateral eyelid and draw tears towards the lacrimal punctum.
In lower motor neuron type of lesion, the frontalis muscle on affected side is weak leading to loss of forehead wrinkles. Ocular signs and symptoms of facial nerve palsy include Lagophthalmos or inability to close the eye, eye redness, tearing, burning, and foreign body sensation.
Eventually the eyebrow descends below the supraorbital rim resulting brow ptosis. Paralytic lagophthalmos and paralytic ectropion or outward turning of lower eyelid from orbicularis weakness are potentially blinding complication that lead to exposure keratitis demand earlier attention.
The most common cause of acquired facial nerve palsy is idiopathic Bell’s palsy followed by iatrogenic causes, infection, trauma, neoplasia, and metabolic causes. The localization of lesion and the cause of palsy are important for subsequent management of the patients.
In facial nerve paralysis there is total loss of nerve function which contrasts with paresis which is a partial loss of nerve function, or incomplete recovery. Patients with mild to moderate paresis have higher rates of recovery than those with severe or complete paresis.1
The synkinesis, which is essentially the development of unwanted or involuntary movements, usually develops if recovery has been prolonged. Aberrant reinnervation after nerve palsy causes synkinesis relevant to the ophthalmologist and include paradoxical frontalis synkinesis (PFS) and buccinator synkinesis. Another synkinesis in facial nerve palsy common in ophthalmic practice is crocodile tears or gustatory lacrimation which is an autonomic synkinesis in which patients tear excessively in response to salivary stimuli.
The ophthalmologists have an important role in managing the symptoms and limiting the sequelae of this condition. Considering the potential for recovery of nerve palsy determines the management of ophthalmic complications either conservative or surgery. Many patients with Bell’s palsy recover fully without intervention.
Medical management in facial nerve palsy – Ophthalmic aspect
In acute phase of facial nerve palsy, conservative management is mostly recommended for all patients whilst waiting for signs of recovery and surgery is reserved for refractory cases with limited potential for recovery. Conservative management include instilling artificial tears, applying lubricating ointment, and taping the eyelids closed or temporary suture tarsorrhaphy (closing the eyes with sutures) that can be removed once the nerve regains function.
Use of Botulinum neurotoxin in facial palsy is a favorable option for causing therapeutic ptosis, reducing crocodile tear production, reducing Synkinesis, minimizing Static Asymmetry, controlling Hyperkinesis.2
Surgical management in facial nerve palsy – Ophthalmic aspect
In long standing cases of facial nerve palsy, there are several indications for oculoplastic surgical treatment in management. Asymmetric face or brow position is cosmetically unappealing that can be corrected by surgery. Incomplete closure of eyelids can be corrected with gravity assisted closure. Lower eyelid ectropion with longstanding corneal exposure can lead to potentially blinding condition. These three conditions are most common in surgical correction in facial nerve palsy.
Surgery for brow ptosis
Direct brow lift is the surgery for the management of brow ptosis to correct the position and symmetry of the brow. Direct brow lifting provides precise repositioning of an asymmetric or ptotic brow, making it applicable in facial aging and facial paralysis.
Case 1, A 73-year-old woman presented with left lower motor neuron type facial nerve palsy. Brow ptosis was noted and surgically corrected by direct brow lift.
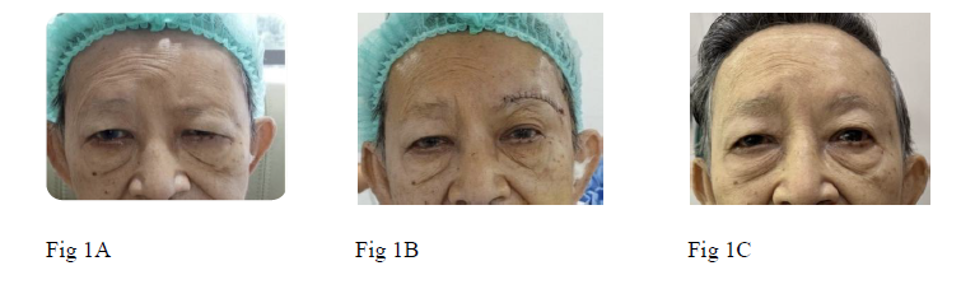
Fig. 1 patient at (A) Preoperative, (B) immediate postoperative, (C) two months after surgery
Surgical correction for paralytic lagophthalmos
Upper eyelid paralytic lagophthalmos can be corrected with upper eyelid loading by providing gravity assisted closure in paralytic lagophthalmos. It is the gold standard treatment. Several materials have been used including stainless steel mesh, tantalum mesh, lead, gold and platinum.
Gold weights are the most popular implant however they have the potential for migration, or extrusion. Poor cosmesis from visibility can be eliminated by placing the implant in higher position than pretarsal fixation. Platinum implants have now superseded gold weights and less post-operative complications. It is not locally available and we have used gold plate for this purpose and achieved good results.
Case 2, 65-year-old lady with left facial nerve palsy presented with incomplete eye closure.

Fig 2. A and B preoperative photos

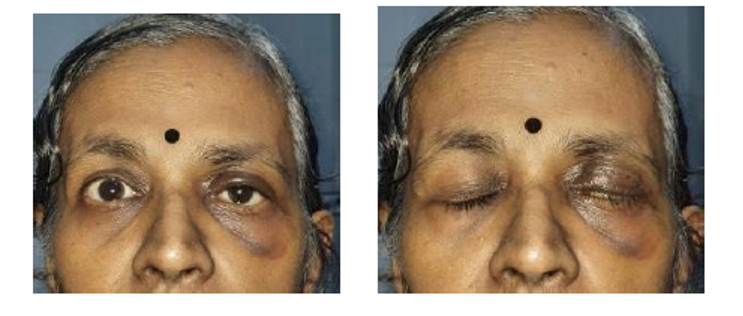
Fig 2. C and D postoperative
Surgery for lower eyelid paralytic ectropion
The lower lid paralytic ectropion has the blinding potential from prolong corneal exposure, subsequently corneal ulceration and perforation. The lower lid ectropion was corrected by tightening of medial canthus with periosteum, suture (5/0 vicryl ) sling and lateral canthal fixation with periosteum of lateral rim.2
Case 3, A 54-year-old-man presented with exposure keratopathy of right eye from paralytic ectropion resulting from longstanding facial nerve palsy.

Fig. 3 A, B preoperative and postoperative
References
1. De Almeida, J.R., Guyatt, G.H., Sud, S., Dorion, J., Hill, M.D., Kolber, M.R., Lea, J., Reg, S.L., Somogyi, B.K., Westerberg, B.D., White, C., Chen, J.M., & Bell Palsy Working Group, Canadian Society of Otolaryngology – Head and Neck Surgery and Canadian Neurological Sciences Federation (2014) Management of Bell palsy: clinical practice guideline. Canadian Medical Association Journal. 186 (12), 917–922. doi:10.1503/cmaj.131801.
2. Okafor, L., Mavrikakis, I. & Malhotra, R. (2024) Facial Palsy. In: F.M. Quaranta Leoni, D.H. Verity, & D. Paridaens (eds.). Oculoplastic, Lacrimal and Orbital Surgery. Cham, Springer Nature Switzerland. pp. 119–145. doi:10.1007/978-3-031-39634-2_11.
Author Information
Khin Ommar Khine,
Consultant Ophthalmologist, Yangon Eye Hospital

