Many couples of reproductive age present to their general practitioner with a delay in achieving conception.Approximately 15% of the population, or 1 in 6-7 couples, experience subfertility, defined as an unwanted delay in conception after 1 year of regular unprotected intercourse.Subfertility could be defined as follows.
Primary subfertility
Delay in conception for a couple who have no previous pregnancy.
Secondary subfertility
Delay in conception for a couple who have conceived previously, even if pregnancy did not end with successful outcome (e.g. miscarriage, ectopic).
Most couples presenting with a fertility problem do not have absolute infertility (i.e. no chance of conception) but rather have relative subfertility with a reduced chance of conception each cycle, due to one or more factors in one or both partners. The major causes of subfertility are ovulation disorders (25%), tubal damage (20%), male factor (30%), uterine or peritoneal disorders (10%). About 25% of cases remain unexplained.
Ideally, the couple should be seen together but there are some problems where one partner should be discussed separately. As a general rule, it is reasonable to start investigations after 1 year of trying, earlier investigations and referral may be justified in women over the age of 35 years after trying to conceive for six months, when an infertility factor is known or when it is highly suspected in the female such as oligo/amenorrhoea, tubal or uterine disease , or endometriosis) or in the male (such as undescended testes) .
Thorough history and examination should be undertaken.
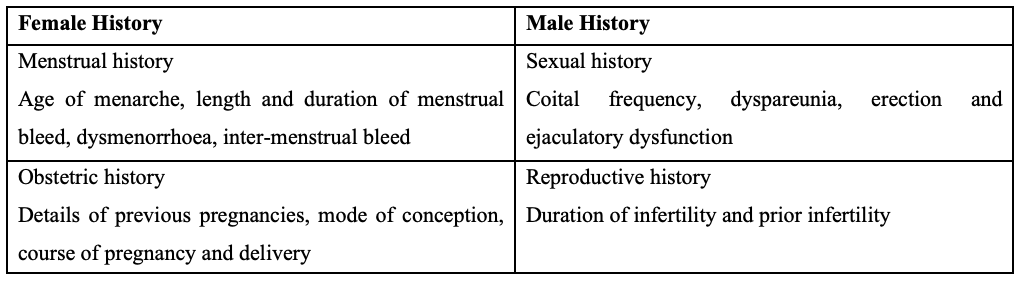
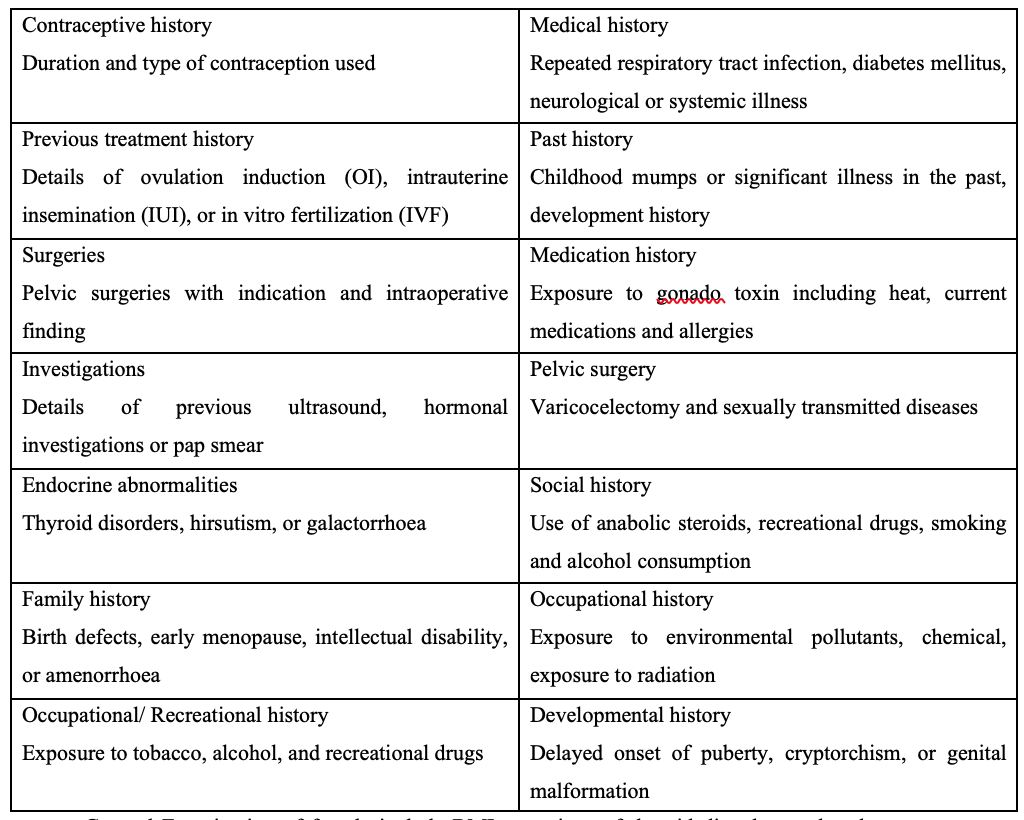
General Examination of female include BMI, any signs of thyroid disorders and androgen excess, hirsutism, breast secretion and insulin resistance. Pelvic examination should also be done. Examination of male includes general appearance and examination of the external genitalia such as presence of varicocele, hernia, vas deferens, epididymis, testicular size and volume, breast examination for gyanecomasia.
Preconceptual counselling
Preconceptual counselling is paramount important as it involves good –practice advice , the aim being to optimise the chance of a good pregnancy outcome for both the mother and the baby.For those with pre-existing medical problems (e.g. Hypertension, diabetes, epilepsy, thyroid disorder, cardiac problems), communicate with appropriate specialist to stabilise these conditions and ensure medical control is optimal. If BMI <20, advise for weight gain and if >30 advise to lose weight. Both partners should be advised to stop smoking and using recreational drugs and reduce alcohol drinking. Frequency of intercourse should be every 2 to 3 days. Folic acid 0.4mg daily is recommended to all low risk women to reduce the risk of neural tube defects, 5mg to those with a history of a previous baby with neural tube defect, who take anti-epileptic medication or are diabetic. Screening for HIV, Hepatitis B &C, syphilis is offered before starting treatment. Chlamydia screening is suggested if available.
Probability of achieving pregnancy naturally depend on the women’s age, previous pregnancy, duration of subfertility, timing and frequency of intercourse, lifestyle factors and cause of subfertility
Making a diagnosis
For natural conception to occur, atleast three elements are required : presence of sperm(of satisfactory quality), presence of (regular or rather regular) ovulation and anatomical integrity of the woman’s pelvis. Therefore, the following basic investigations are required, 1. semen analysis, 2. assessment of ovulation, 3. a tubal patency test.
1. Semen analysis
It is an appropriate starting point in the investigation of male partner. Sample should be collected after 2-7 days of sexual abstinence, preferably at the fertility clinic by masturbation. It could also be collected with condom without chemical additives and delivered to the laboratory within an hour of collection.
If first semen analysis is abnormal, repeat confirmatory test should be done ideally 3 months after the initial analysis, to allow time for the cycle of spermatozoa formation tobe completed. If a gross spermatozoa deficiency (azospermia or oligospermia) has been detected, the repeat tests should be undertaken as soon as possible.
If repeat semen analysis reveal – severe oligo<5 million spermatozoa /ml or azospermia, serum FSH, LH, testosterone and oestradiol should be measured. Prolactin is only tested in men who complain of reduced libido and low testosterone.
2. Diagnosis of ovulation
Single progesterone measurements of 15nmol/L suggest ovulation occurs, 30nmol/L confirms ovulation. The best time to measure is 7 days before expected period (mid-luteal phase of their cycle).).Ovulation could also be assessed by follicular tracking by transvaginal scan and urine LH kits. For Irregular cycles, blood test (FSH & LH) should be done.
3. For tubal patency, the following tests could be done.
(1) Laparoscopy and dye test,
(2) HSG (Hysterosalpingogram),
( 3) (SIS) Saline infusion ultrasonography
These should be performed optimally within 10 days of a menstrual period, preferable after the period of active bleeding, when the risk of pregnancy is reliably excluded.HSG is recommended as the primary screening procedure in low risk patients. Laproscopy should be considered in patients with a history suggestion of endometrosis, previous PID or pelvic surgery.
4. Diagnostic tests for uterine factor
(1) Hysterosalpingogram: Evaluates uterine cavity for abnormalities.
(2) Hysteroscopy: Gold standard test for identifying uterine anomalies. The other advantage is the potential to immediately treat any intracavitary lesion.
An initial semen analysis and progesterone measurement is typically undertaken by the general practitioner (primary care). Any remaining tests are undertaken in the setting of a fertility clinic that is run by fertility specialist (Secondary Care).
Unexplained infertility
A diagnosis of exclusion when a woman is not pregnant after 12 months of frequent unprotected sexual intercourse, when there is evidence of regular ovulation and her partner has normal concentration of motile sperm. Young couple should be advised to keep trying for up to 2 years. Ovarian stimulation agents like anti-oestrogens (clomiphene citrate and tamoxifen) or aromatase inhibitors (letroz) are not useful treatments .If not conceived after 2 years of trying, they should be referred for IVF.
Management (Prognostic based approach)
Nowadays, a more prognostic –based approach is moving from a diagnostic approach For example, repeated semen analyses indicate severe male factor subfertility requiring IVF/ICSI treatment which does not depend on the natural function of ovulation or the patency of the fallopian tubes. In that case, performing these investigations are not expected to influence decision making, only tests relevant to IVF (ovarian reserve tests) are required.
1. Medical Treatment
(A) For Women
For an ovulatory or oligo- ovulatatory women (hypothalamic pituitary dysfunction such as PCOS), clomiphene citrate, as the first line of treatment, could be given (50mg daily from D2-D5 of the menstrual cycle) for 5 days. It is an antioestrogen agent to induce gonadotrophin release by occupying the oestrogen receptor in hypothalamus, there by interfering with normal feedback mechanism. Raised FSH stimulates the ovary to produce more follicles. It could be used maximally 6 months. Seventy percent of those taking this drug will ovulate and 15-20 % will become pregnant. The risks are multiple pregnancy,(10-20 %), ovarian hyper stimulation syndrome and ovarian cancer.
Tamoxifen could also be used as ovulation induction agent (2.5- 5 mg /day starting from day 2- 3 of menstrual cycle for 5 days). FSH or HMG (human menopausal gonadotrophin) could be used alone or combine with clomiphene for ovulation induction. For women with hyperprolactinaemic amenorrhoea, dopamine agonist such as bromocriptine help regain normal ovulation.
(B) For Men
Men with idiopathic semen abnormalities should not be offered antiestrogens, gonadotrophins, androgens, bromocriptine or kinin-enhancing drugs because they have not been shown to be effective. Hypogonadotrophic hypogonadism has been successfully treated with injection of human chorionic gonadotrophin orpulsatine administration of GnRH (gonadotrophin releasing hormone).Anti-oxidant could be used to reduce oxidative stress which impair semen parameter (still debatable).The use of bromocriptine in men wih sexual dysfunction as a result of hyperprolectinemia is effective.
2. Surgical Treatment
(A) For Women
Women with moderate or severe endometriosis should be offered surgical treatment because it includes the chance of pregnancy. For female with mild tubal diseases, tubal surgery may be more effective than no treatment. If underlying causes are uterine factors, they should be treated, for examples, myomectomy for myoma, polypectomy for endometrial polyp, excision for uterine septum.
(B) For Men
Varicocelectomy does not seem to be an effective treatment for male or unexplained subfertility. For obstructive azospermia, the options are PESA (Percutaneous Sperm Aspiration), TESE (Testicular Sperm Extraction), TESA (Testicular Sperm Aspiration).
3. ART (Assisted Reproductive Techniques) are Timed Sexual Intercourse (TSI), Intrauterine Insemenation (IUI) and IVF ( Invitro Fertilization ) +/- ICSI ( Intracytoplasmic sperm insemination)
(a) TSI (Timed Sexual Intercourse)
It is suitable for anovulatory cycle, patent fallopian tubes with mild male factor. Three to six cycles may be tried depending on patient’s age and response to ovulation induction drugs.
(b) IUI (Intrauterine Insemenation)
It is suitable for mild male factor (sperm count > 10million /ml), patent both tubes, previous failed timed intercourse. Success rate is about 10-15 %. It is simple, cost effective and minimally invasive procedure. It should not be done in case of cervical atresia, cervicitis and endometritis. The complications are infection, multiple pregnancy miscarriage and ectopic pregnancy.
(c) IVF (Invitro Fertilization)
It is recommended for those with blocked both tubes, moderate to severe endometriosis, oligoasthenospermia, obstructive azospermia, failed IUI and unexplained infertility. Success rate varies with various fertility centers. – The risks are OHSS, injury to bowel, bladder and vessels, pelvic infection and multiple pregnancy.
References
- NICE Clinical Guideline 156(2013). Fertility : Assessment and Treatment for People with Fertility Problems.
- Nandi N & Homburg R. Unexplained subfertility: diagnosis and management. The Obstetrician & Gynaecologist. 2016; 18, 107 – 15.
- Chaitra Nayak (2018) “Infertile couple-initial investigations” in kaminiARao (ed.)The Infertility Manual. New Delhi. Jaypee Brothers Medical Publishers,p.26
- Yakoub Khalif (2016) “Male infertility” in David M.Luesley and Mark D.Kilby (eds),“An Evidence-based Text for the MRCOG, 3rdEd”.London.Tayler& Francis Group, LLC,P638-642
- Yakoub Khalif (2016) “Female infertility” in David M.Luesley and Mark D.Kilby (ed),“An Evidence-based Text for the MRCOG, 3rdEd”.London.Tayler& Francis Group, LLC,P629-637
Dr. Yu Yu Moe1 Dr. Mee Mee Thet2
Senior Consultant, Fertility Center, Central Women’s Hospital, Yangon
Associate Professor, Fertility Center, Central Women’s Hospital, Yangon