
Background
Headache is very common medical complaint. It can be a symptom of an illness as well as a disease itself; in the former case, we have to work up to recognize underlying sinister causes to give specific treatment, and in the latter case, if we can diagnose correctly, it is easily manageable with preventive and symptomatic medications. Here we will focus on approach to various types of headache.
Causes of Headache
Common primary headache syndromes
- Migraine
- Tension type headache
- Cluster and other trigeminal-autonomic cephalgias
- Trigeminal neuralgia
Important secondary causes of headache are
- Hemorrhage (intracranial, subdural, subarachnoid)
- Infections (meningitis, encephalitis, abscess, subdural empyema)
- Vascular disorders (e.g. vascular malformations, vasculitis, venous sinus thrombosis)
- Brain space occupying lesion (SOL),
Other causes of headache are
- Dental disorders, sinusitis, glaucoma
- Giant cell arteritis,
- Analgesics overuse
- Low pressure headaches (Cerebrospinal fluid leak)
- Idiopathic intracranial hypertension
Evaluation
Evaluation of headache should start with determining primary or secondary headache. Unless the headache is chronic and intermittent, check the red flags for serious secondary causes.
Five red flags suggesting secondary causes of headache are
- Obtundation of sensorium
- Focal neurological signs and symptoms including visual abnormality, meningism
- Signs and symptoms of raised intracranial pressure
- Constitutional symptoms such as fever, loss of appetite and loss of weight
- Special characters of headaches such as headache that develops within minutes (thunderclap headache), new onset headaches in > 50 years old, persistent/ prolonged/ progressive headaches, change in character from previous headache, being awakened by headache, worsen with changing posture/ exertion/ coughing/ straining, associated with jaw claudication.
After history and examination, diagnosis of secondary causes of headache should be individualized by putting into consideration of patient’s context to guess the etiology of headache. e.g., headache in the patient with HIV would indicate opportunistic CNS infection, headache in the patient with risk factors for thrombosis (e.g. puerperium) may suggest cerebral venous thrombosis, headache in the patient with severe hypertension (SBP > 220 mmHg or DBP > 120 mmHg) might suggest intracranial hemorrhage after combining with respective red flags. All these will guide to necessity of further management such as hospital admission, checking inflammatory markers, scans (CT/MRI/MRV), CSF study, blood culture, etc and treatment is finally directed at the cause.
Indications for CT or MRI in a headache patient (1)
- Thunderclap headache
- Altered mental state
- Meningism
- Papilloedema
- Signs of sepsis
- Acute focal neurological deficit
- Severe hypertension (SBP > 220 mmHg or DBP > 120 mmHg on consecutive readings)
If no cause or serious symptoms and signs are identified and headache is intermittent or chronic, focus the evaluation on diagnosing primary headache disorders.
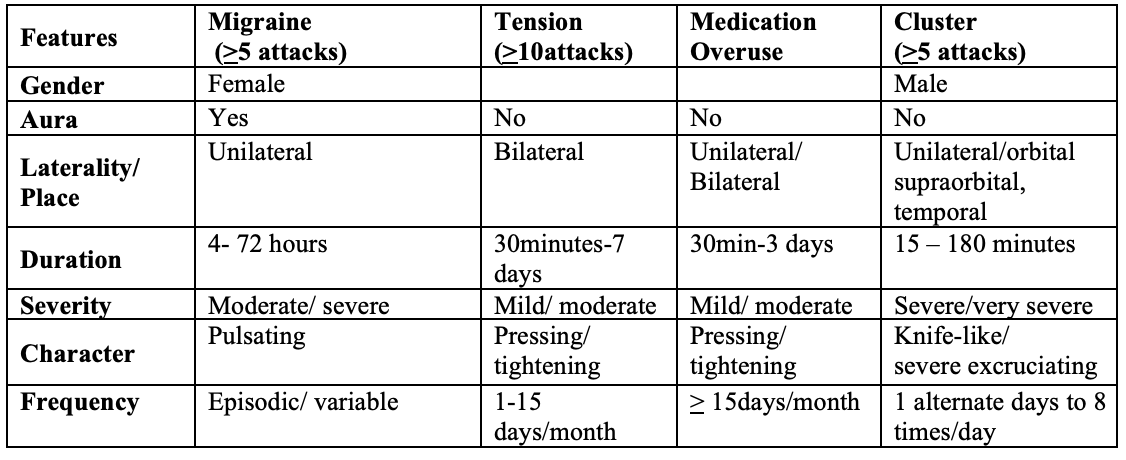
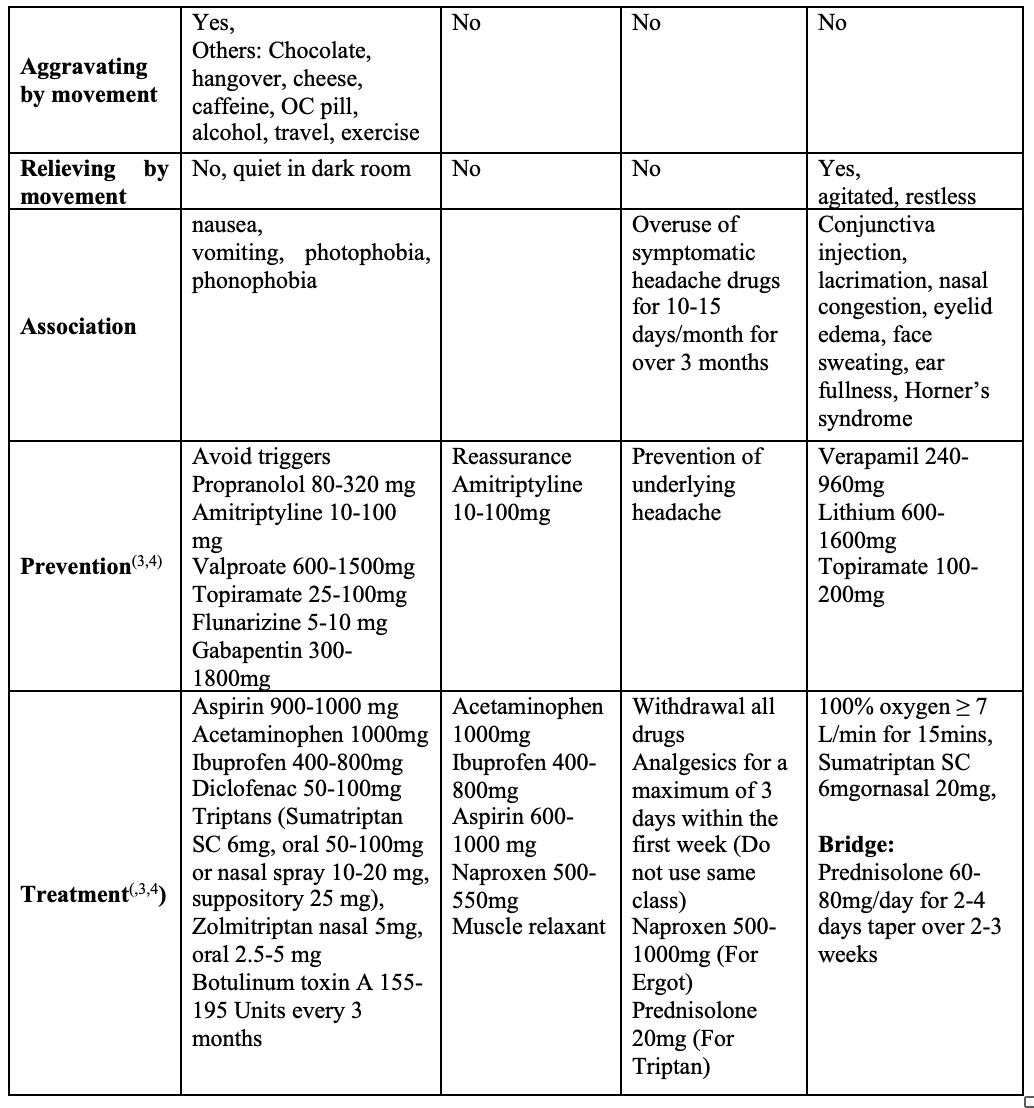
Common chronic headaches and their characteristics (2)
Common case scenarios of headache encountered in clinical practice
Case 1.A 25-year old lady presented with 5-year history of recurrent hemi cranial headache, around four times/month, each lasting for around 4-6 hours and the attacks were sometimes severe affecting her work. It was associated with nausea,vomiting and photophobia. Examination was normal and there were no red flags. This is a case of migraine without aura. We can prescribe propranolol as preventive medication if no contraindication and acetaminophen as symptomatic treatment when the attacks come.
Case 2: A 45-year old lady had pressing headache at vertex for six months, which did not affect her work and daily life. Each attack lasted half an hour to one hour and it normally went away without any medication. It occurred mostly in the afternoon and nearly ten times a month. It was not associated with nausea,vomiting, phonophobia and photophobia. This is a case of frequent episodic tension-type headache and we can prescribe amitriptyline as preventive medication.
Case 3: A 51-year-old man presented with 2-month history of severe left supraorbital pain, 2-3 times a day, each attack lasting about one hour and associated with ipsilateral lacrimation, rhinorrhea, and ptosis. Clinical examination and MRI (brain) were normal. This is a case of cluster headache. We can prescribe 100% oxygen and sumatriptanas acute treatment, prednisolone over fourteen days as bridging, and verapamil as preventive medication.
Case 4: A 42-year old man presented with intense unilateral electric shock like pain at left cheek without tooth or sinus problem and no sensory loss (numbness) at that area. This is a case of trigeminal neuralgia and carbamazepine or oxcarbamazepine can be started with close monitoring for Steven-Johnson syndrome.
Case 5: A 30-year old lady, 2 weeks postpartum, presented with new onset headache associated with 2-time seizures. Her D-dimer was raised and CTVconfirmed cerebral venous thrombosis (CVT). Her symptoms were resolved after treatment of the CVT.
Case 6: A 56-year oldman with known history of hypertension presented with sudden onset severe thunderclap headache. On examination, GCS was 15 but he had neck stiffness and BP was 180/110. CT (head) urgent revealed subarachnoid hemorrhage (SAH). He was managed with lowering BP to safer level to avoid re-bleed and other SAH management.
Case 7: A 38-year old lady with pre-existing migraine developed a new type of headache which was significantly worse than her pre-existing headache. Frequency was 15 times a month and she was taking analgesics nearly every day. This is a case of medication-overuse headache, and it resolved after the overuse was stopped.
Conclusion
Headache is very common and sometimes it is challenging to the primary care provider to evaluate and manage. Red flags must be screened to decide for the need of neuroimaging and to recognize underlying sinister causes for secondary headache. Chronic intermittent headaches are usually benign and are primary headache syndromes. If these are frequent, preventive treatment and follow up for the response are necessary.
Acknowledgement
Author is grateful to Prof T. Umapathi (National Neuroscience Institute, Singapore) for his bedside guidance on approach to headache during the training days.
Disclosure
There is no conflict of interest and no financial grant from any organization or individual.
References
- Singh, G., Gupta, P., Gupta, A., &Khanal, M. Clinical approach to a patient with headache. Medicine Update. India: API India, 2013; 514-518
- Arnold, M. Headache classification committee of the international headache society (IHS) the international classification of headache disorders. Cephalalgia, 2018; 38(1), 1-211
- Becker, W. J., Findlay, T., Moga, C., Scott, N. A., Harstall, C., &Taenzer, P. Guideline for primary care management of headache in adults. Canadian Family Physician, 2015; 61(8), 670-679.
- Jensen, R., Valade, D., Savi, L., Lainez, M. J. A., Diener, H. C., Martelletti, P Couturier EG; European Headache Federation; Lifting The Burden: The Global Campaign to Reduce the Burden of Headache Worldwide; World Health Organization. European principles of management of common headache disorders in primary care. Journal of Headache and Pain, 2007; 8, 3.
Ohnmar1, Kyawt Oo Kay Thi Htay2, Sai Kyaw Win3, Khin Myat Po Po Kyaw4, Yin Minn Aye5, San Oo6
- Associate Professor, Department of Neurology, University of medicine 1
- Specialist Assistant Surgeon, Department of Neurology, Yangon General Hospital
- Assistant lecturer, Department of Neurology, University of medicine 1
- Consultant Neurologist, Department of Neurology, Yangon General Hospital
- Associate Professor, Department of Neurology, Yangon General Hospital
- Professor, Department of Neurology, University of medicine 1
Primary author’s information:
Dr. Ohnmar, Associate Professor, Department of Neurology, University of medicine 1.
M.B.B.S (Ygn), M.Med.Sc (Int Med), MRCP (UK), FRCP (Edin), Dr.MedSc (Neurology)
Email: dr.maohmar@gmail.com, Phone: 095198124




