Introduction
Hyperimmunoglobulin E syndrome (HIES) or Job syndrome is a rare primary immunodeficiency disorder occurring in one in one million individuals.1 It is characterized by a classical triad of high immunoglobulin E (Ig E) levels, repeated pulmonary infections and recurrent cold skin abscesses from Staphylococcus infections.2 There are two forms of HIES, autosomal dominant and autosomal recessive forms. Majority of autosomal dominant HIES (AD-HIES) have been found to be due to mutations in STAT3, whereas DOCK8 mutations have been identified in patients with autosomal recessive HIES (AR-HIES). Although patients with AD-HIES have distinct dental, skeletal and connective tissue abnormalities, these features usually appear during late childhood and also not found in patients with AR-HIES. STAT3 mutations have been found in many ethnic groups with an equal gender distribution.3 Here, we report a five-year-old boy with hyper Ig E syndrome presenting with a retropharyngeal abscess.
Case Report
A five-year-old boy was admitted to Yankin Children’s Hospital with a month history of dysphagia and a week history of noisy breathing. He had been referred from one of the regional hospitals. He had no history of fever. Three weeks ago, he was seen by a local pediatrician and oral antibiotics were started. However, there was no significant improvement and he was unable to eat or drink. In addition, he developed breathing difficulty and noisy breathing. Therefore, he was seen by a consultant otolaryngologist and lateral neck X-ray was done. It showed retropharyngeal abscess. Then he was referred to Yankin Children Hospital.
Interestingly, since the age of two months, he had a history of skin lesions like atopic dermatitis requiring frequent visits to general practitioners. Since seven months of age, he had been suffering from recurrent respiratory tract infections including empyema requiring thoracotomy and chest tube insertion. Furthermore, he also had multiple skin abscesses on and off for years. The parents denied any contact with tuberculous patients. He was admitted to both local hospital and one of the tertiary children’s hospitals many times. He needed several courses of antibiotics and topical steroid previously.
He is a product of unrelated parents. He was born by normal delivery at full term. Both parents and his older siblings are healthy. His immunization status is up-to-date as per Myanmar EPI regime.
On examination, he was quite small with both height and weight below third percentile. He looked quite drowsy. He had inspiratory stridor, severe suprasternal and intercostal indrawing. Air entry was generally poor in both lungs and a few crackles were heard in the right upper and middle zones. He had bilateral cervical lymphadenitis and multipleold scars. The rest of the examination was normal.

Fig.1. Erythematous papules, macules and excoriation of skin
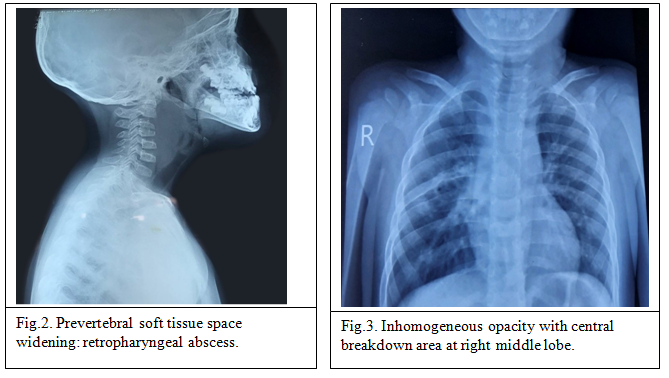
Lateral neck X-ray showed significant widening of the prevertebral soft tissue space compactable with retropharyngeal abscess. Chest X-ray revealed inhomogeneous opacity with central breakdown at right middle lobe.
Full blood count showed neutrophil leucocytosis, mild hypochromic microcytic anaemia and normal platelet count. His inflammatory marker levels were high with ESR of 50 mm after the first hour and C-reactive protein level of 120 mg/L.
He was put on intravenous amoxicillin and flucloxacillin. The pediatric surgical team was involved in the management of the boy. Emergency laryngoscopy, incision and drainage were proceeded under general anaesthesia. About 50 ml of pus was obtained and it was sent for culture and sensitivity. Moderate growth of Staphylococcus sensitive to both amoxicillin and flucloxacillin was insolated. Intravenous antibiotics were given for two weeks and he responded well.
Because of significant recurrent infections, he was screened for both primary and acquired immunodeficiency syndromes. Serum for HIV antibody was non-reactive. His immunoglobulin levels revealed sky high Ig E level (> 2500 IU/ ml (ref.< 100 IU/ml), normal Ig G, Ig A and Ig M levels.
In view of severe atopic dermatitis, recurrent pulmonary infections, frequent skin abscesses, and extremely high Ig E level, he was finally diagnosed as hyper Ig E syndrome (also called Job syndrome). Genetic study for HIES is unable to do in Myanmar.
He was discharged with prophylactic antibiotics (oral flucloxacillin) to cover staphylococcal infections and was referred to dermatology team. He will be reviewed by our team and local pediatric team regularly.
Discussion
HIES is a rare syndrome characterized by atopic dermatitis, frequent skin and sinopulmonary infection together with markedly elevated Ig E levels. In our patient, he presented with severe atopic dermatitis, repeated skin abscesses, frequent episodes of chest infections and extremely high level of Ig E levels. Most of autosomal dominant HIES patients have characteristic skeletal and connective tissue abnormalities, our patient did not have those features as he was still young and those features only appear during late childhood period. Although the majority of cases reported from other countries had eosinophilia, our patient had no eosinophilia. Eosinophilia is not an essential criterion for the diagnosis of HIES. Genetic testing should be carried out to confirm the diagnosis of HIES. Because of financial hardship and unavailability of these genetic tests in Myanmar, we are unable to confirm the diagnosis.
Conclusion
Although, primary immunodeficiency disorders are rare, they should be considered in children who present with unusual frequent infections. If a child presents with atopic dermatitis, recurrent skin abscesses and repeated chest infections, Ig E level should be checked to get the diagnosis of hyper Ig E syndrome. Both adequate treatment of infections and prophylactic antimicrobial agents should be considered individually.
- Ghaffari J, Ahanchian H, Zandieh F. Update on hyper IgE syndrome (HIES), J Pediatr Rev 2 (2014) 39–46.
- Hashemi H, Mohebbi M, Mehravaran S, Mazloumi M, Jahanbani-Ardakani H, Abtahi SH. Hyper immunoglobulin E syndrome: genetics, immunopathogenesis, clinical findings, and treatment modalities. J Res Med Sci 2017; 22:53.
- Patrick FK Yong, Alexandra F Freeman, Karin R Engelhardt, Steven Holland, Jennifer M Puck and Bodo Grimbacher. An update on the hyper-IgE syndromes. Arthritis Research & Therapy 2012, 14:228.
Author Information
Aung Khin Thein1, Aye Yu Yu Mon2
- Associate Professor/ Consultant Paediatrician, Yankin Children Hospital
MBBS, M. Med.Sc (Paed), MRCPCH, FRCPCH - Specialist AS (Pediatrics), Yankin Children Hospital
MBBS, M. Med.Sc (Paed)