Introduction
In 1900, Dr. Walther Petersen, a German surgeon, first described Petersen space hernia which is an internal hernia caused by the Petersen defect, a space between the Roux limb and the transverse mesocolon formed after Roux-en Y (R-Y) reconstruction.1 This is a rare internal hernia that can occur after any type of gastrojejunostomy.1
The herniation of either afferent or efferent limb could become strangulated and lead to acute necrosis, leading to severe infection and sepsis. Short bowel syndrome may result even after surgical correction. As a consequence, the death rate of Petersen’s hernia could reach 30%.2
Internal hernia has been recognized as a potential complication of R-Y gastric bypass (RYGBP), with an incidence of 1–5 % in open surgery during the past decade. Studies for complications after RYGBP have reported a significantly higher incidence of long-term internal hernia after laparoscopic surgery than open surgery. 3
Petersen’s hernia is a life-threatening complication after gastro-jejunostomy in gastric cancer or bariatric surgery. This study is a case report about herniation after gastro-jejunostomy for gastric volvulus and diaphragmatic hernia.
Case report
In April 2023, a 43-year-old farmer complained of colicky abdominal pain in the whole abdomen, constipation, abdominal distension and vomiting for one day.
He had history of open surgery for diaphragmatic hernia with intestinal obstruction in May 2021. Laparotomy was done and diaphragmatic hernia repair, decompression, adhesiotomy, splenectomy and chest tube insertion were carried out.
A year later, in April 2022, he suffered abdominal pain and underwent a second laparotomy for gastric volvulus and adhesive intestinal obstruction for which adhesiotomy and gastrojejunostomy were carried out.
On general examination, he was dehydrated and urine output was reduced. On examination of the abdomen, there was marked tenderness and guarding and bowel sound reduced. Per-rectal digital examination revealed empty rectum.
Plain-X-ray of the abdomen showed dilated small bowels. (Figure 1)
Blood investigations showed hyperglycaemia and leucocytosis. Viral screening also revealed Hepatitis B antigen positive.
Laparotomy was carried out after optimizing the patient. Small gut mesentery was twisted clockwise due to herniation of all the jejunum and ileum through the window behind the gastrojejunostomy. The jejunum and ileum were cyanotic due to the herniation and twisting. There was a moderate amount of hematoma in the mesentery. (Figure 2)
During the surgery, jejunum and ileum were reduced back through the window behind gastrojejunostomy, caecum was fixed to lateral peritoneal wall, appendicectomy was done, gastrojejunostomy was fixed to transversemesocolon, jejuno-jejunostomy was done between afferent and efferent limbs.
Decompression was carried out by Ryle’s tube suction. (Figure 3)
Drain was inserted into pelvis and wound was closed back by mass closure.
Early surgical intervention was carried out in this case and small bowel gangrene was avoided.
Discussion
Petersen hernia is a specific type of hernia where the small bowel moves into the potential space between the caudal surface of the transverse mesocolon and the edge of the Roux limb. Petersen hernia is rarer than other internal hernias that have mesocolon mesentery defects and jejunojejunostomy after R-Y reconstruction.4
The clinical presentation ranges from mild and intermittent abdominal cramping to acute small bowel obstruction (SBO). The most feared complication of IH is strangulation. SBO is a serious complication, with a reported prevalence 0⋅6–11 per cent.5
Diagnostic challenge can present in Petersen’s hernia and can result in late intervention and complications. Early diagnosis is essential to prevent gangrene of herniated intestine.
Petersen’s hernia can develop after any gastric operation with gastro-jejunal anastomosis. Early diagnosis and treatment are utmost important to prevent intestinal gangrene. Defect closure can significantly reduce the incidence of small bowel obstruction.
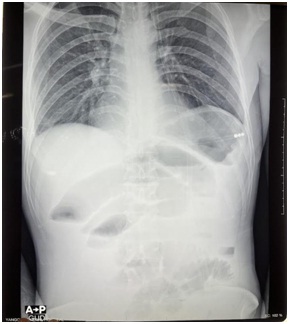
Fig1– Plain-X-Ray of abdomen (erect) showing dilated small bowels
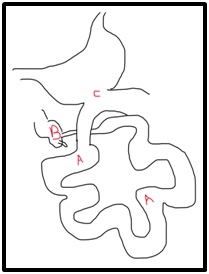
Fig 2– Diagram showing the intraoperative findings; A – dilated jejunum and ileum, B – high-riding caecum, C – previous gastro-jejunostomy

Fig 3– Ryle’s tube output after reduction of hernia and untwisting the small intestine
References
- Petersen W. (1900) “Concerning Twisting of the Intestines Following a Gastroenterostomy”. Langenbecks Arch Klin Chir 62:94–114.
- Yoshikawa K, Shimada M, Kurita N, Sato H, Iwata T, Higashijima J, et al. (2014) “Characteristics of Internal Hernia After Gastrectomy With Roux-En-Y Reconstruction for Gastric Cancer”. Surg Endosc 28(6):1774–8. doi: 10.1007/s00464-013-3384-7
- Paroz A, Calmes JM, Giusti V, Suter M. (2006) “Internal hernia after laparoscopic Roux-en-Y gastric bypass for morbid obesity: a continuous challenge in bariatric surgery.” Obes Surg.;16:1482–7.
- Garza E Jr, Kuhn J, Arnold D, Nicholson W, Reddy S, McCarty T (2004) “Internal hernias after laparoscopic Roux-en-Y gastric bypass.” Am J Surg 188:796–800
- Koppman JS, Li C, Gandsas A. (2008) “Small bowel obstruction after laparoscopic Roux-en-Y gastric bypass: a review of 9527 patients.” J Am Coll Surg; 206: 571–584
Author Information
Sie Thu Myint1&2, Zin May Win3, Khin Hsu Hlaing1&2, Aung Myat1&2, Htun Thuya1&2, Thein Lwin1&2
1. Department of surgery, University of medicine (1), Yangon,
2. Surgical Ward 2, Yangon General Hospital
3. Academy Hospital