HFpEF has been a very topical subject in the last few years. Most physicians do not clearly understand until recently and is the most common form of heart failure in our day to day practice. Prognosis is same as Heart failure with reduced ejection fraction.
Heart failure with preserved ejection fraction (HFpEF) previously, HFpEF termed “diastolic HF.” is a clinical syndrome in patients with current or prior symptoms of HF with a left ventricular ejection fraction (LVEF) ≥50 percent and evidence of cardiac dysfunction as the cause of symptoms (eg, abnormal LV filling pattern and elevated filling pressures) 1,2.
Clinical Manifestations
The clinical manifestations of HFpEF are generally the same as those for other forms of HF (eg, HF with reduced ejection fraction [HFrEF])3,4. Dyspnoea (including dyspnoea on exertion, paroxysmal nocturnal dyspnoea, and orthopnea) and fatigue are the most common symptoms of HFpEF5. Exertional chest pain is also a common presentation in patients with HFpEF.6
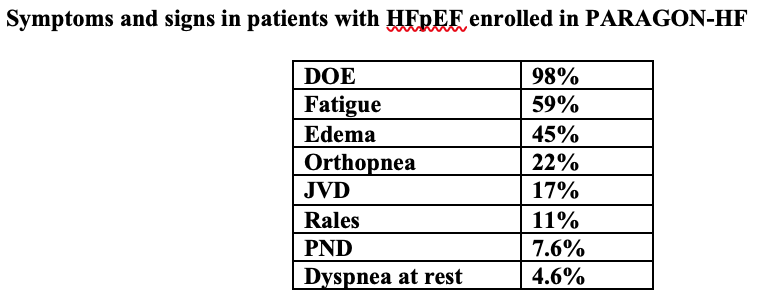
HFpEF: heart failure with preserved ejection fraction; DOE: dyspnea on exertion; JVD: jugular vein distention; PND: paroxysmal nocturnal dyspnoea.
When to suspect HFpEF — We suspect HFpEF if the history or physical examination reveal at least one symptom of HF that is not sufficiently explained by another diagnosis. In patients with symptoms of HF, the presence of certain conditions increases the likelihood that HFpEF is present:
- Age ≥60 years
- Obesity
- Hypertension
- Coronary artery disease
- Atrial fibrillation (AF)
- Diabetes
- Chronic kidney disease
Pathophysiology>
Endothelial and vascular dysfunction in HFpEF — Obesity, insulin resistance, hypertension, and aging are frequently observed comorbidities in HFpEF that are believed to play an important role in the pathophysiology. One common thread that binds these comorbid conditions together and may explain many of the findings in HFpEF is endothelial dysfunction7. Endothelium-dependent vasodilation is impaired in HFpEF, and the presence and severity of endothelial dysfunction is associated with more severe HF symptoms, worse exercise capacity, and higher event rates 8,9.
Neurohormonal activation is the main pathophysiology of HFrEF but less significant in HFr EF.
Hypertension, obesity, insulin resistance, and sedentary lifestyle — Chronic increases in left ventricular afterload induced by systemic hypertension may lead to concentric remodeling or hypertrophy that predisposes to HFpEF. This may be related to fibrotic changes in the cardiac interstitium or changes in the cardiac myocytes themselves 10. This form of concentric remodeling in HFpEF was formerly thought to be related to hydraulic stress alone, but studies suggest that comorbid conditions related to obesity and insulin resistance create a proinflammatory milieu that may predispose to ventricular remodeling and stiffening above and beyond what is seen with high blood pressure alone.
A theoretical framework has been proposed in which comorbidities (such as hypertension, overweight/obese, diabetes mellitus, chronic obstructive pulmonary disease, sedentary lifestyle, and iron deficiency) create a systemic inflammatory state that causes coronary microvascular endothelial dysfunction leading to HFpEF 10,11. A proinflammatory state causes coronary microvascular endothelial cells to produce reactive oxygen species that reduce nitric oxide bioavailability, which in turn decreases protein kinase G activity in cardiomyocytes. Low protein kinase G activity disinhibits cardiomyocyte hypertrophy and results in cardiomyocyte stiffening due to hypophosphorylation of the cytoskeletal protein titin. Coronary microvascular endothelial cells also produce vascular cell adhesion molecule and E-selectin, which promote migration of monocytes into the subendothelium. Transforming growth factor beta released by monocytes stimulates conversion of fibroblasts into myofibroblasts that deposit collagen in the interstitial space.
Further study is needed to better define the potential role of inflammation and associated alterations in HFpEF and, importantly, to define whether targeting these factors can improve clinical status and outcomes.
Initial testing — The initial evaluation of patients with suspected HFpEF commonly includes the following tests:
- Chest radiograph – A chest radiograph is commonly obtained in patients with HF to assess for signs of pulmonary oedema and identify other causes of dyspnea. The chest radiograph may show cardiomegaly with or without evidence of pulmonary edema. Most patients with HFpEF have a normal chest radiograph11. Thus, normal chest radiography does not exclude HFpEF.
- ECG – An electrocardiogram (ECG) is routinely performed in patients with HF, although the findings are often nonspecific. Evidence of myocardial ischemia or prior infarction may be present. AF is observed in approximately 40 to 50 percent of patients with HFpEF, and the lifetime risk of AF in patients with HFpEF is approximately 67 percent12. The presence of AF on ECG in a patient with normal LVEF and dyspnea increases the odds that HFpEF is present by more than 20-fold 13.
- Echocardiography– If echocardiography has not been performed, we obtain a complete Doppler echocardiogram. Echocardiography can identify abnormal diastolic function and other causes of HF (eg, pericardial disease, valve disease), and is required to calculate the H2FPEF score.
Key measures obtained by echocardiography include:
- Left ventricular ejection fraction– The presence of an LVEF ≥50 percent is required for the diagnosis of HFpEF.
- Pulmonary artery systolic pressure– Elevation in pulmonary artery systolic pressure (PASP) estimated by echocardiography is common in patients with HFpEF, and the identification of an elevated PASP in an older patient with dyspnea raises suspicion for the diagnosis of HFpEF14. PASP >35 mmHg is a criterion of HFpEF diagnostic scores.)
- Signs of abnormal diastolic function and elevated filling pressures– Echocardiography can be used to measure functional parameters suggestive of diastolic dysfunction (eg, E/e’ ratio) that support the diagnosis of HFpEF. The approach to echocardiographic assessment of diastolic dysfunction is discussed separately. (See “Echocardiographic evaluation of left ventricular diastolic function in adults”.)15The findings of left atrial enlargement or concentric LV remodeling or hypertrophy can support the diagnosis of HFpEF or lead the clinician to suspect HFpEF but are not necessary to reach the formal diagnosis of HFpEF. If structural parameters cannot be adequately measured by echocardiography, we suggest obtaining cardiovascular magnetic resonance imaging, although slight differences in measures among imaging modalities have been reported16.
Goals of therapy — For patients with HFpEF, the goals of treatment are to reduce HF symptoms, increase functional status, and reduce the risk of hospital admission. There is no clear evidence that pharmacologic therapy, diet, or other therapies reduce the risk of mortality in patients with HFpEF.
Exercise, diet, weight loss, and cardiac rehabilitation — In patients with HFpEF, participation in structured exercise programs, cardiac rehabilitation, and dietary interventions is safe and can lead to small improvements in exercise tolerance. The role of exercise, diet, weight loss, and cardiac rehabilitation in the management of patients with HFpEF is discussed separately.
Conditions commonly associated with HFpEF include hypertension, atrial fibrillation (AF), coronary artery disease, hyperlipidemia, obesity, anemia, diabetes mellitus, chronic kidney disease (CKD), and sleep-disordered breathing 17. In general, these conditions are managed using approaches similar to those used to treat the general population or other forms of HF; there is no evidence for HFpEF-specific management of these conditions.
Pharmacotherapy
Preferred therapies for symptomatic patients — The following therapies are most likely to reduce the risk of HF hospitalization and/or improve HF symptoms in patients with HFpEF compared with other therapies.
Patients with volume overload — Patients with HFpEF and suspected or documented volume overload require diuretic therapy before initiating other pharmacologic therapies. The type and dose of loop diuretics depends on the severity of volume overload.
In stable patients with HF, negative balances for sodium and potassium are greatest during the first few days of loop diuretic therapy (with most sodium losses typically occurring after the first dose). The time required to achieve a new steady state (when sodium and potassium excretion equals intake) depends on the amount of fluid overload at the start of therapy, but it averages two weeks).
Once a new steady state is reached, continued diuretic therapy will maintain the fluid loss that has been attained but will not induce further fluid or potassium loss unless the dose is increased, a second type of diuretic is added, or there is a change in HF severity or sodium intake. Thus, monitoring of serum electrolyte levels is warranted if the diuretic regimen is augmented or changes in HF severity or sodium intake are suspected.
The risk of hypokalemia is reduced by concurrent treatment with an aldosterone antagonist. When used for diuresis or potassium sparing effects, higher doses of spironolactone may be needed.
SGLT2 inhibitors – In trials that included patients with HFpEF, SGLT2 inhibitors reduced the risk of HF hospitalization and improved quality of life but did not clearly reduce the risk of mortality. The benefit of SGLT2 inhibitors must be weighed against the risk of recurrent urinary tract infections and genital infections.
MRA – In trials that included patients with HFpEF, MRAs reduced the risk of HF hospitalization but did not clearly reduce the risk of mortality. The benefit of MRA therapy must be weighed against the risk of hyperkalemia.
Secondary therapies — We do not routinely use the following medications for the treatment of HFpEF, though ACE inhibitors and ARBs are used as first-line therapy for patients with diabetes and CKD. Compared with the preferred therapies for HFpEF listed above, these medications do not clearly reduce the risk of HF hospitalizations.
Sacubitril-valsartan – For patients with HFpEF and LVEF ≤55 percent whose volume status is well-treated with diuretics but who have persistent HF symptoms and evidence of poorly controlled blood pressure (ie, >135/80 mmHg) despite optimal SGLT2 inhibitor and MRA therapy, we suggest sacubitril-valsartan as an additional blood pressure therapy.
Most of the physicians including cardiologists are not familiar with prescribing new medications together in the treatment of HFpEF. Actually, these new medications are safe and effective in treatment of HFpEF.
I have been working along with advanced heart failure team in my clinical practice. So, I am familiar with all new medications used in heart failure (both HFrEF or HFpEF). The more we understand the pathophysiology, we are more comfortable with prescribing new medications such as SGLT 2 inhibitors together with diuretics, MRA and ARNI which will become standard treatment for HF in general in the future. Needless to say. We all need to emphasize the importance of compliance with medications, salt and water restriction and exercise as tolerated.
References
- Pfeffer MA, Shah AM, Borlaug BA. Heart Failure With Preserved Ejection Fraction In Perspective. Circ Res 2019; 124:1598.
- Zile MR. Heart failure with preserved ejection fraction: is this diastolic heart failure? J Am Coll Cardiol 2003; 41:1519.
- Aurigemma GP, Gaasch WH. Clinical practice. Diastolic heart failure. N Engl J Med 2004; 351:1097.
- Baicu CF, Zile MR, Aurigemma GP, Gaasch WH. Left ventricular systolic performance, function, and contractility in patients with diastolic heart failure. Circulation 2005; 111:2306.
- Borlaug BA, Redfield MM. Diastolic and systolic heart failure are distinct phenotypes within the heart failure spectrum. Circulation 2011; 123:2006.
- Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37:2129
- Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013; 62:263.
- Borlaug BA, Olson TP, Lam CS, et al. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. J Am Coll Cardiol 2010; 56:845.
- Akiyama E, Sugiyama S, Matsuzawa Y, et al. Incremental prognostic significance of peripheral endothelial dysfunction in patients with heart failure with normal left ventricular ejection fraction. J Am Coll Cardiol 2012; 60:1778.
- Paulus WJ, Tschöpe C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013; 62:263.
- Schiattarella GG, Altamirano F, Tong D, et al. Nitrosative stress drives heart failure with preserved ejection fraction. Nature 2019; 568:351.
- Reddy YNV, Carter RE, Obokata M, et al. A Simple, Evidence-Based Approach to Help Guide Diagnosis of Heart Failure With Preserved Ejection Fraction. Circulation 2018; 138:861.
- Zakeri R, Chamberlain AM, Roger VL, Redfield MM. Temporal relationship and prognostic significance of atrial fibrillation in heart failure patients with preserved ejection fraction: a community-based study. Circulation 2013; 128:1085.
- Reddy YNV, Obokata M, Gersh BJ, Borlaug BA. High Prevalence of Occult Heart Failure With Preserved Ejection Fraction Among Patients With Atrial Fibrillation and Dyspnea. Circulation 2018; 137:534.
- Lam CS, Roger VL, Rodeheffer RJ, et al. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol 2009; 53:1119.17 Pieske B, Tschöpe C, de Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J 2019; 40:3297.
- Pieske B, Tschöpe C, de Boer RA, et al. How to diagnose heart failure with preserved ejection fraction: the HFA-PEFF diagnostic algorithm: a consensus recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur Heart J 2019; 40:3297.
- Mentz RJ, Kelly JP, von Lueder TG, et al. Noncardiac comorbidities in heart failure with reduced versus preserved ejection fraction. J Am Coll Cardiol 2014; 64:2281.
Author Information
Dr Thaung Han Myint MD
Attending physician
Tampa, Florida