
The use of cannabis as medicine is emerging now and the use of cannabinoids are restricted and disallowed in many countries. Limited evidence suggests cannabis can reduce nausea and vomiting during chemotherapy, improve appetite in people with HIV/AIDS, and reduce chronic pain and muscle spasms.
The medicinal use of the cannabis plant dates back to thousands of years in many cultures. Followed by regulatory and scientific review, medical organizations now have requested the removal of cannabis from the list of controlled substances. However, our country and our medical organization is not in this category
Cannabis administration is possible through various methods: capsules, lozenges, tinctures, dermal patches, oral or dermal sprays, cannabis edibles, and vaporizing or smoking dried buds. Synthetic cannabinoids is also available by prescription in some countries. Currently, countries that allow the medical use of whole-plant cannabis include: Australia, Canada, Chile, Colombia, Germany, Greece, Israel, Italy, the Netherlands, Peru, Poland, Portugal, and Uruguay.
Nausea and vomiting
Medical cannabis has been shown to be effective in chemotherapy-induced nausea and vomiting. Comparative studies have shown that cannabis is more effective than conventional antiemetics such as prochlorperazine, prome-thazine, and metoclopramide.
Pain
When inhaled, blood levels of cannabinoids rise faster than oral products, peaking within three minutes and attaining an analgesic effect in seven minutes. A 2011 review considered cannabis to be safe and appears safer than opioids in palliative care.
History
William Brooke O’Shaughnessy, an Irish physician, is credited with introducing cannabis to western medicine. Noting in particular its analgesic and anticonvulsant effects, O’Shaughnessy returned to England with a supply of cannabis in 1842.
Cannabis began to attract renewed interest as medicine in the 1970s and 1980s, particularly with for cancer and AIDS patients who reported relief from chemotherapy effects and wasting syndrome. In 1996, California became the first US state to legalize medical cannabis in defiance of federal law. In 2001, Canada became the first country to adopt a system regulating the medical use of cannabis.
Countries that have legalized the medical use of cannabis include Australia, Canada, Chile, Colombia, Croatia, Cyprus, Czech Republic, Finland, Germany, Greece, Israel, Italy, Jamaica, Luxembourg, Macedonia, Malta, the Netherlands, Peru, Poland, Portugal, the United Kingdom, and Uruguay. Other countries have more restrictive laws allowing for the use of specific cannabinoids only, such as Brazil and France which have approved the use of Sativex. Countries with the most relaxed laws include Canada, Uruguay, the Netherlands, and Spain, where cannabis can be obtained without a prescription. In Mexico, THC content of medical cannabis is limited to one percent. The same limit applies in Switzerland but no prescription is required for purchase. In the United States, the legality of medical cannabis varies by state.
Medical organizations
Medical organizations have issued statements in support of allowing access to medical cannabis include: the American Nurses Association, American Public Health Association, American Medical Student Association, National Multiple Sclerosis Society, Epilepsy Foundation, and Leukemia & Lymphoma Society.
Other organizations that have issued statements in oppositon to the legalization of medical cannabis include the American Academy of Pediatrics, American Psychiatric Association, and American Society of Addiction Medicine. However, the AAP also supports rescheduling for the purpose of facilitating research.
The American Medical Association and American College of Physicians do not take a position on the legalization of medical cannabis, but have called for the Schedule I Classification of cannabis to be reviewed. The American Academy of Family Physicians similarly does not take a position , but does support rescheduling in order to facilitate research. The American Cancer Society and American Psychological Association have noted the obstacles that exist for conducting research on cannabis, and have called on the federal government to better enable scientific study of the drug.
Most countries want to use cannabis as a pain relieving drug for patients with intractable cancer pain. With the view of increasing patients and improved cancer treatment in our country, it is high time we do not miss the wagon.
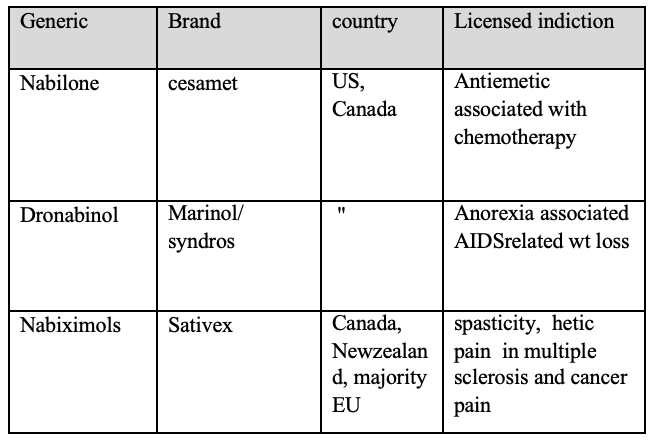
Following is a list of drugs used in limited scope in some countries.
Dr. Ye Win
MBBS, MMedSc(Physiology)
Former teacher at IM2, IM1