Childhood overweight and obesity is one of the emerging health concerns worldwide. Together with increasing trend of childhood obesity, there is an emergence of young people with serious comorbid conditions like insulin resistance, metabolic syndrome, type 2 diabetes, hypertension, fatty liver conditions and hyperlipidemia. The problem is global and increasing dramatically in many low and middle income countries, especially in the urban setting. According to WHO data, in 2016 the number of overweight children under five is estimated to over 41 million , almost half of the overweight children under five lived in Asia and one quarter live in Africa(5). Overweight and obese children are more likely to become overweight and obese adults and more likely to develop non communicable diseases like diabetes, cardiovascular diseases, stroke and other costly health conditions and serious burden for country. In Yangon 7.6% of the children and adolescent aged 10-19 years were obese in both sexes. (4)
In determining the etiology and diagnosis of obesity, a number of factors have been identified. The most important factors are: changing food pattern, sedentary lifestyle, maternal and paternal overweight and intrauterine conditions. The main causative factors are food choices, high fat and carbohydrate diet, knowledge and lifestyle practices. Parental obesity influences children overweight and obesity because of genetic factors, family environment and influence of food choices. Factors such as maternal obesity, insulin resistance and diabetes can affect intrauterine conditions for the fetus. Other intrauterine conditions can lead to low birth weight, IUGR, and high birth weight which is associated with rapid catch up growth, early adiposity rebound and possibly obesity in adulthood. Longitudinal study in Finland involving 4032 children from 12thweek of gestation to 16 years of age was conducted. The risk of obesity and overweight at 7 -16 years of age strongly correlated with parental BMI, maternal gestationaldiabetes , excessive weight gain in pregnancy , maternal smoking in pregnancy and birth weight . It is inversely correlatedwith parental professional (especially maternal) and socioeconomic status in children. (1)
For the diagnosis of childhood obesity, body mass index and body mass index percentile, growth chart from WHO and CDC are used. The Endocrine Society clinical practice guideline for children more than two years is: overweight (from > 85th percentile to <95th percentile), obese (> 95th percentile) and extremely obese (>120%of the 95% or 35kg/M2).The diagnosis of a child less than 2 years of age as obese is if the sex specific weight for recumbent length is more than 97th percentile on WHO charts. It is recommended to plot and review a child’s or adolescent‘s BMI percentile at least annually during well child and /or sick child visit. In overweight and obese children, waist circumference is useful and measured at a level mid way between the lowest rib and iliac crest. This provides an index of visceral adiposity and correlates well with metabolic complications. (3)
In evaluating an overweight or obese child, athrough history and physical examination is important. The following should be explored: detail birth history, medical illness, drug history, family life style and dietary pattern. The checklist should include:
a. Weight, height, and BMI calculation
b. Blood pressure (interpret using height /weight percentile )
c. Acanthosis nigricans, acne , skin tag , hirsutism in prepubertal girl
d. Thyroid examination
e. Tanner staging
f. Any bone deformity e.g. , short fourth metacarpal
g. Eye examination
h. Any clinical feature of syndromic obesity and systemic examination
i. Any neurodevelopmental abnormality
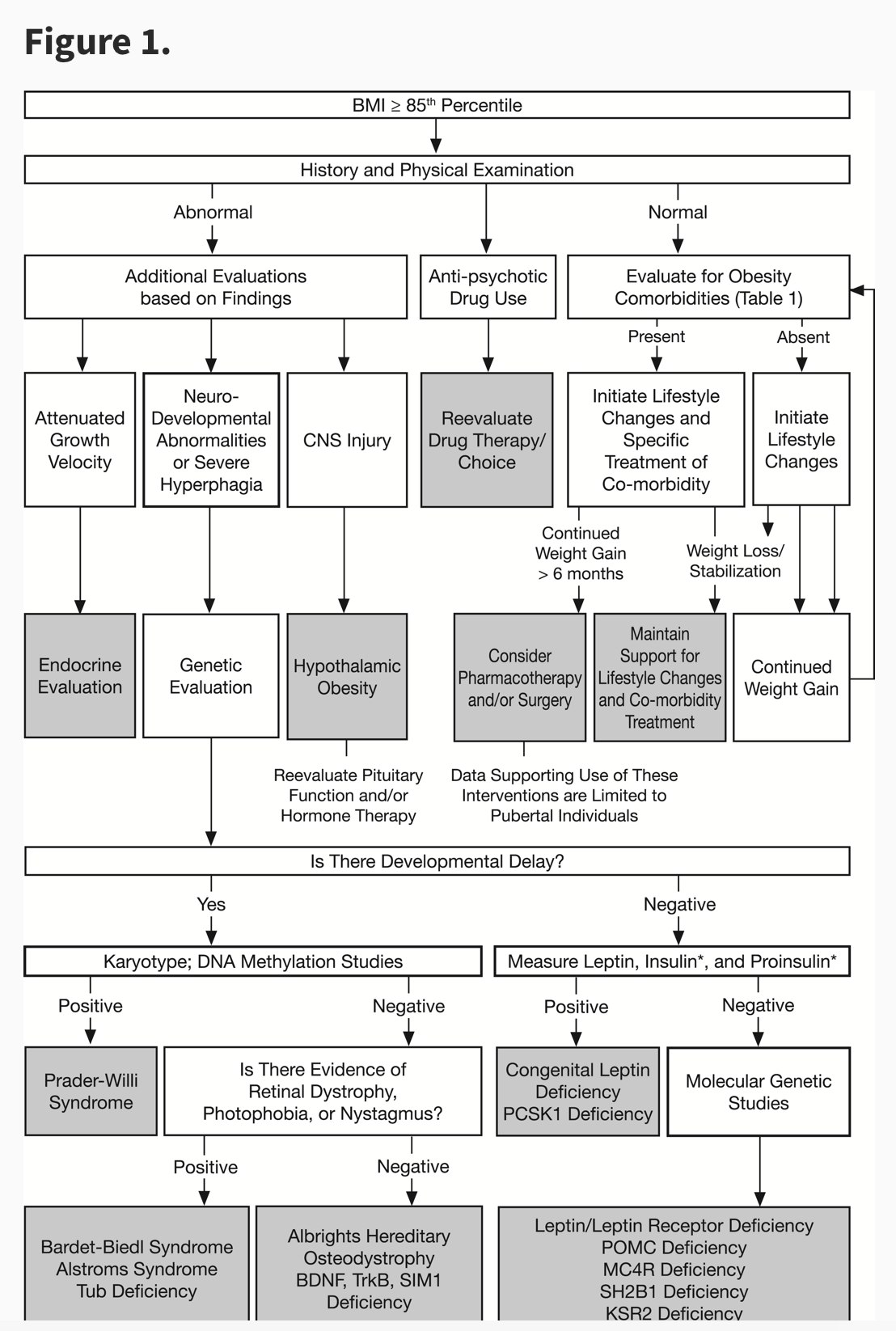
The following flowchart of management of an obese child from the Endocrine Society guideline is useful for clinician evaluation. The screening of comorbid conditions in overweight and obese child is essential in management of the child. (See Flow Chart 1).
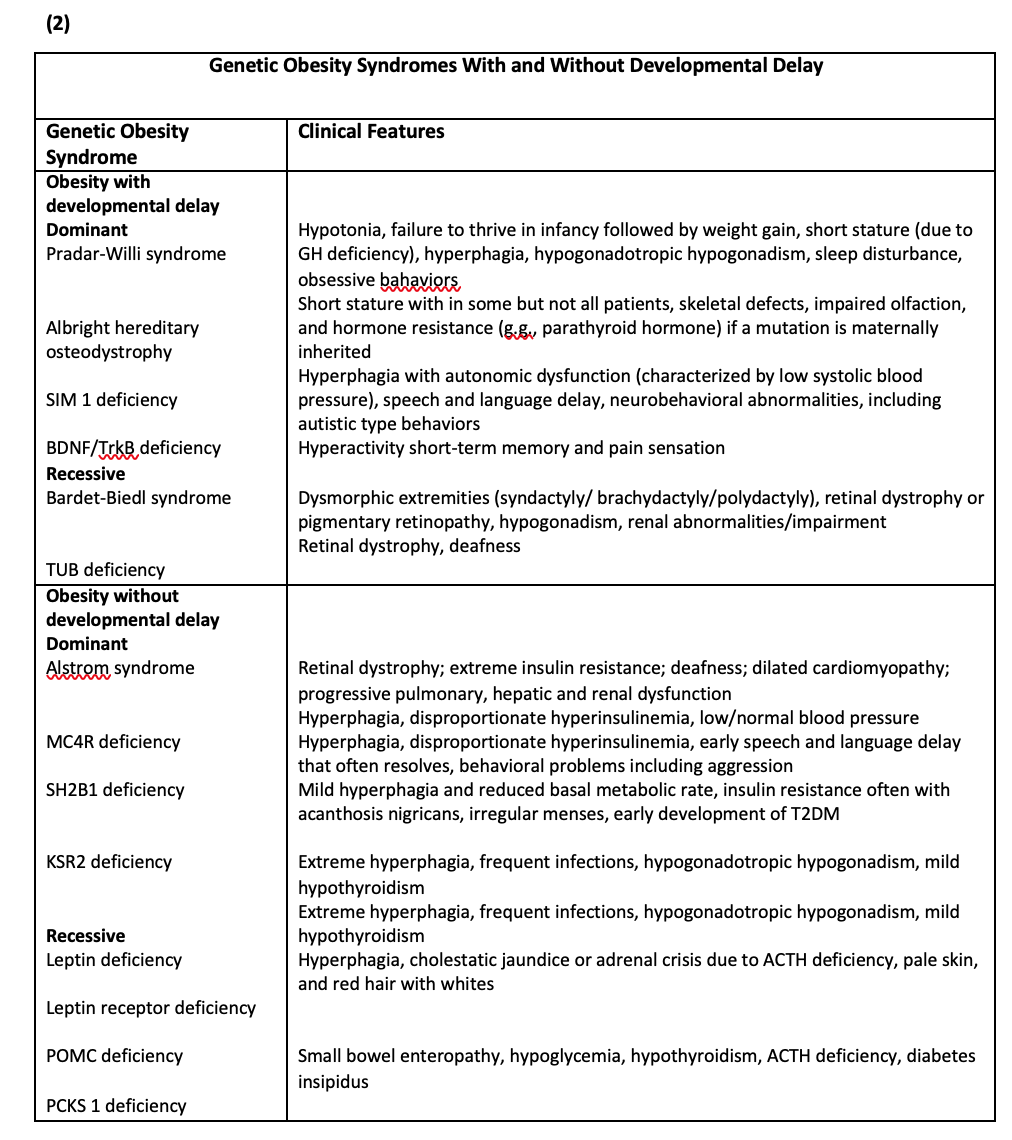
The genetic cause of obesity in children is not uncommon conditions especially in evaluation if children under two years of age present with overweight and obesity. In table 1 the important causes of genetic obesity are described. (From Endocrine Society Guideline).So, it’s important to have any developmental abnormality in evaluating the child is important.
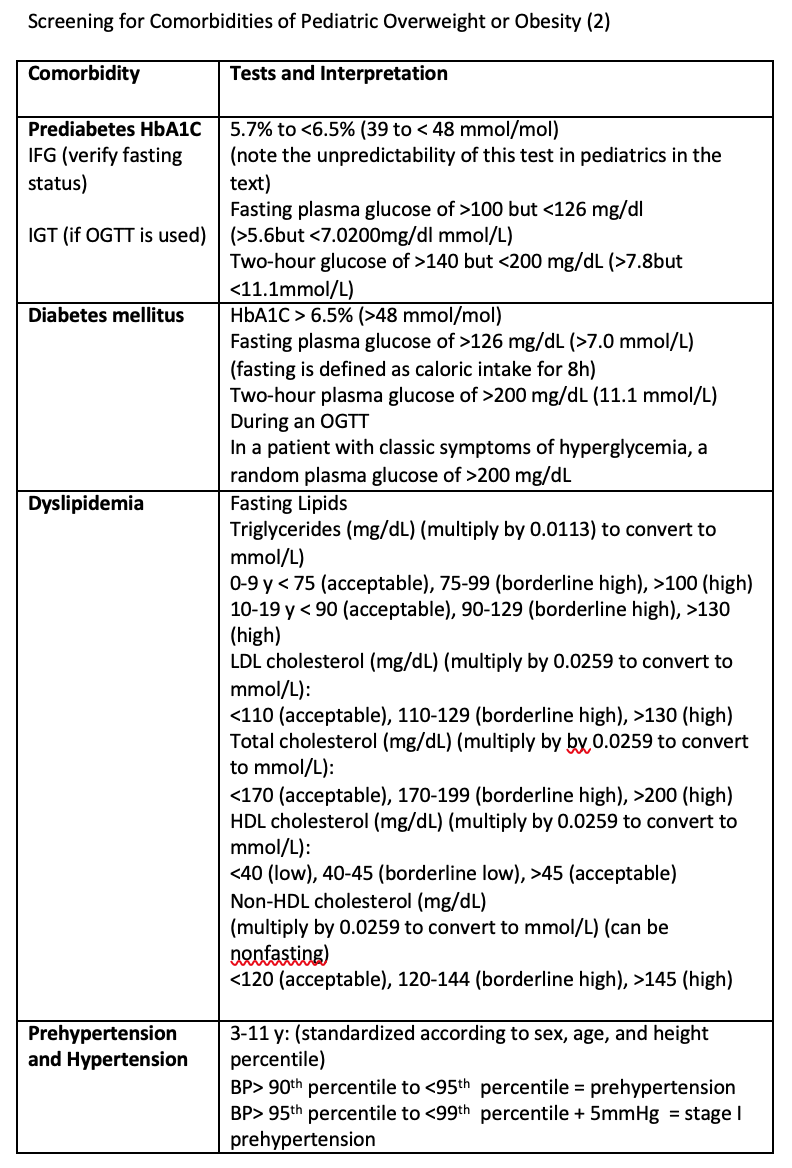
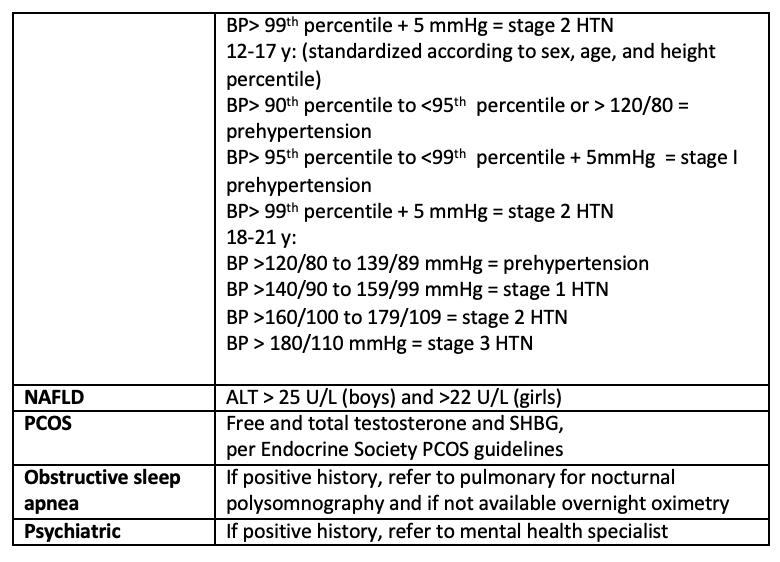
The childhood overweight and obesity is the starting point of many adulthood diseases. The psychosocial low esteem, low school performance , bone condition like slipped upper femoral epiphysis are the short term complications The long term complications include metabolic syndrome, insulin resistance, type 2 diabetes, nonalcoholic cirrhosis, hypertension , hyperlipidemia and cardiovascular risk in young adult. The obesity and cancer positive association like endometrial cancer , breast cancer are not uncommon conditionWhen a clinician see a child with overweight or obesity , it’s important to screen whether the comorbid conditions are present or not.
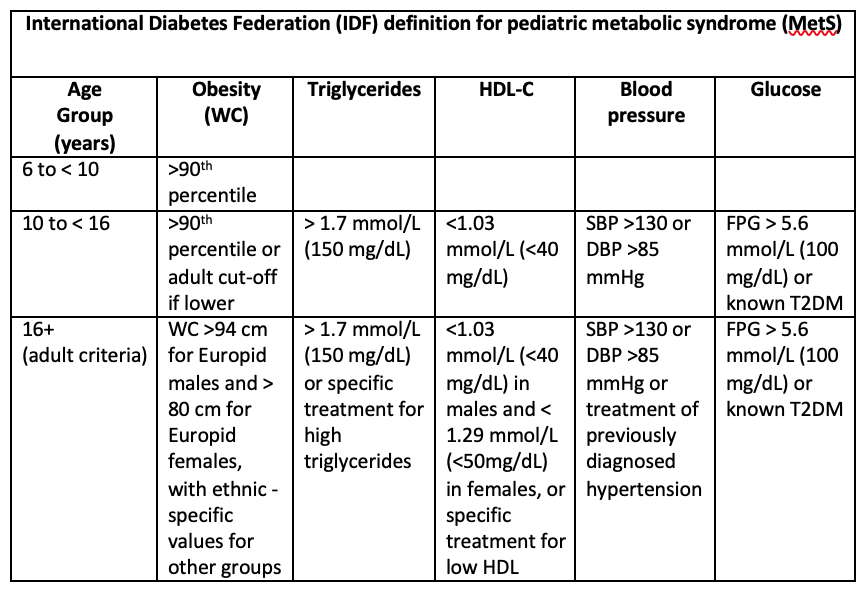
In diagnose of metabolic syndrome in children, we can use the criteria from IDF as follow.( Table 2)
Treating Obesity in children
The basic managentis to have negative energy expenditure .The energy intake should be reduced and physical activity should be increased. The behavior changing community based program, active participating and family support is essential. The changing habit and intensive life style modifications is a great challenge for the children. But sustain and effective weight control measures must be needed. Among the pharmacotherapy use in adult obesity , only orlistat is approved for use in children ages 12 to 16 years Orlistat reduced intestinal fat absorption by 30% but it has significant side effect. (2) The indications for bariatric surgery are as follows.
- The patient has attained Tanner stage 4 or 5 and reach near or final adult height
- The patient has BMI more than 40kg/m2 or BMI 35kg/m2 and having significant comorbid conditions and fail to intensive life style modifications with or without pharmacotherapy
- The patient should have access to experienced surgeon and a team capable of long term follow up and have family support is import in decision making to have bariatric surgery.(2)
In conclusion, obesity in child hood contributes to many diseases burden in adult hood. Prevention obesity in childhood is the essential measure to reduce the disease burden that can be based on food policy, school food environment, child hood family based and community based program, environment measure are essential.
References
- Brownell KD, KershR,LudwigDS,et al, (2010)Personal Responsibility and Obesity :aconstructive approach to a controversial issue .Health Aff ( Millwood):29(3):379-87
- Dennis M. Styne,Silva A. Arslanian,Ellen L. Connor ( 2017) Pediatric Obesity—Assessment, Treatment,and Prevention: An Endocrine SocietyClinical Practice Guideline, J ClinEndocrinolMetab, March 2017, 102(3):709–757
- Michael S Freemark (2018 ), Pediatric Obesity : Etiology , Pathogenesis and Treatment ,2nd Edition .New York USA, Humana Press
- Tint SweLatt ,KoKo , Than Than Aye (2011) , Summary of Myanmar Clinical Guideline for Management of Obesity ,ASEAN Endocrine Journal, 78-379
- WHO, (2014), Global Statue Report on Non communicable Disease