

High blood pressure is a risk factor for various cardiovascular diseases and non-cardiovascular diseases other than common presentations of stroke and ischaemic heart disease (IHD). Stroke and IHD occurs in young adult to very elderly age groups and determine the prognosis. In elderly and very elderly age groups, hypertensive cardiomyopathy leads to heart failure with preserved diastolic function (HFpEF) and heart valve consequences.
The consequences of hypertension can be divided into two groups, in young adult to very elderly age group – stroke, IHD, death and exclusively in elderly and very elderly age groups – HFpEF, aortic syndromes, aortic stenosis and dementias. [1]
Stroke
Hypertension remains the single most important modifiable risk factor for stroke, and the impact of hypertension and nine other risk factors together account for 90% of all strokes in INTERSTROKE study. [2]More of the cases had ischemic stroke than intracerebral hemorrhagic stroke 78% versus 22%.History of hypertension was the strongest risk factor for stroke, with nearly a threefold increased risk and the association was stronger for hemorrhagic stroke. [3]
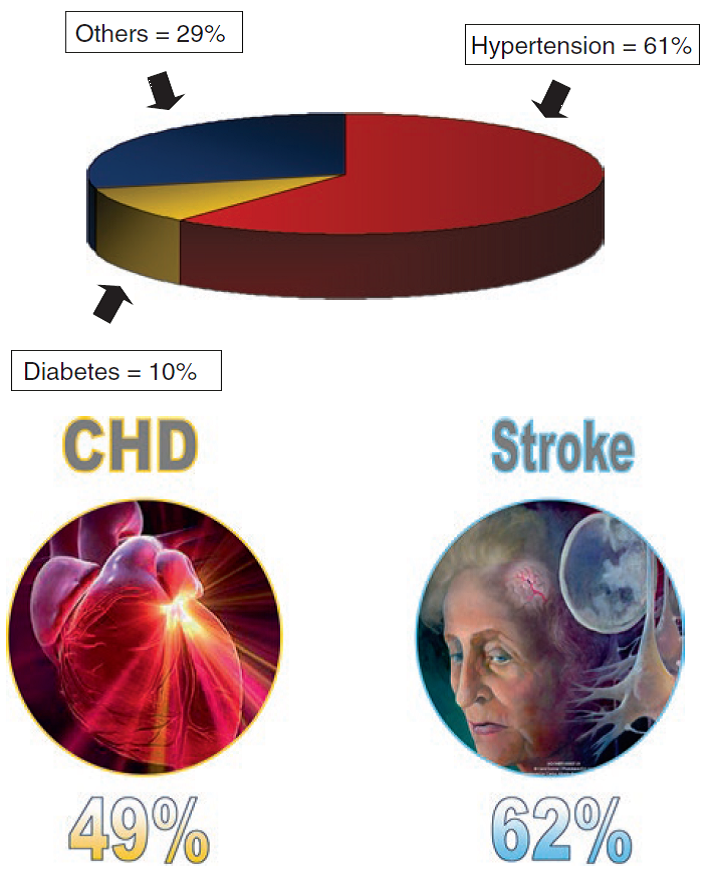
Fig: Risk attributable to IHD and Stroke estimated by WHO [4]
70–80% of strokes can be prevented by reducing blood pressure with antihypertensive drug treatment, e.g. 30/15mm Hg. [5]
Ischaemic heart disease
Hypertension is a major risk factor for ischaemic heart disease (IHD). Among the numerous risk factors associated with IHD, hypertensionplays a major role given its high frequency and its physiopathogenesis. Thus, roughly 15% of the general adult population manifest hypertensionwith a net male predominance, and 25% of patients with IHD have hypertension. IHD is the first cause of morbidity and mortality in hypertensive patients. [6]
Although hypertension alone is weakly predictive of individual risk for the occurrence of IHD but the association between the level of blood pressure and the risk of IHD is independent of other factors.
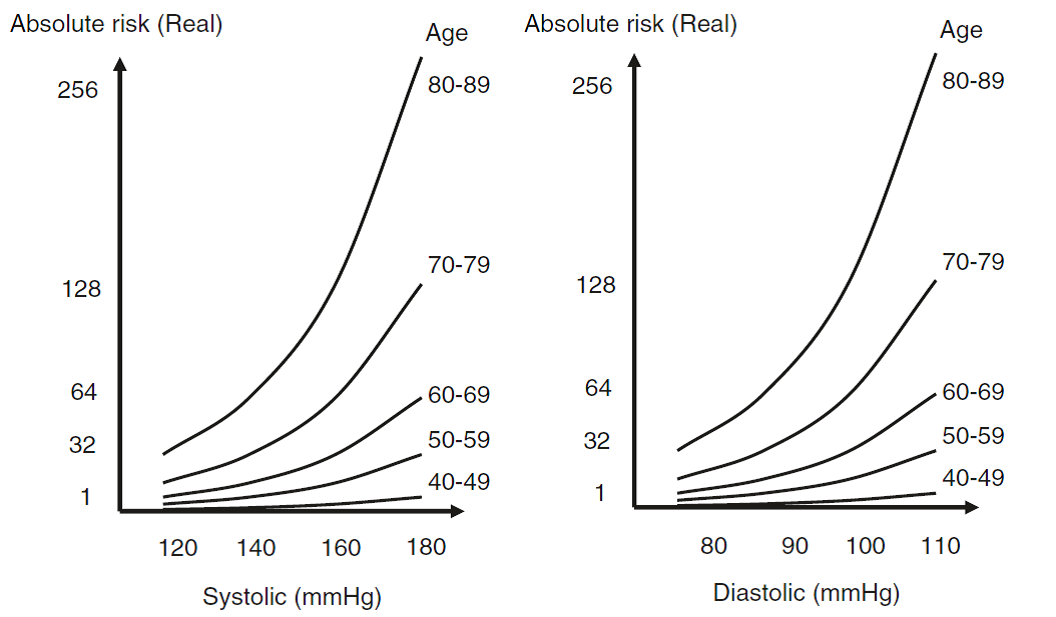
Fig: Absolute risk for IHD and Stroke according to BP level and age groups [1]
Hypertensive cardiomyopathy
Hypertensive cardiomyopathy (HTN-CM) is a structural cardiac disorder generally accompanied by concentric left ventricular hypertrophy (LVH). Persistent systemic hypertension leads to structural and functional myocardial abnormalities resulting in myocardial ischemia, fibrosis, and hypertrophy. HTN-CM is predominantly a disease of impaired relaxation rather than impaired contractility, so patients are usually asymptomatic during resting conditions. However, their stiff left ventricles become incapable of handling increased blood volume and cannot produce appropriate cardiac output with the slight change of circulating volume that may occur during exercise. [7]
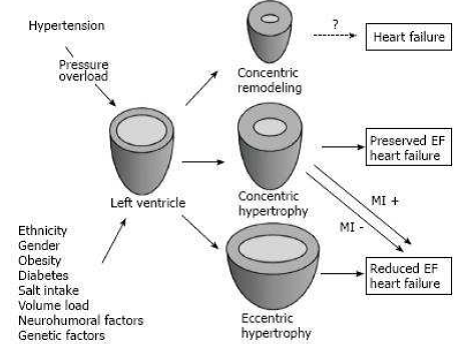
Fig: Pathways of left ventricular remodeling progression secondary to systemic hypertension [7]
Heart Failure
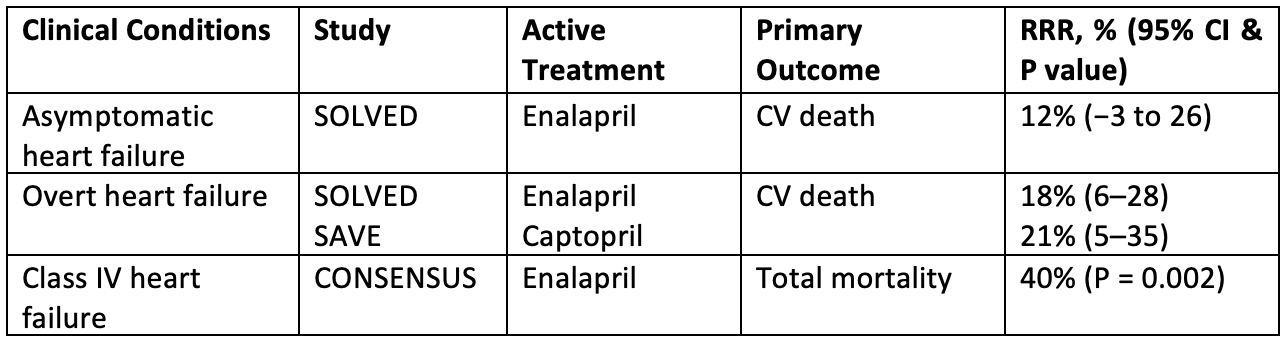
Both heart failure with reduced ejection fraction (HFrEF) and HFpEF are common in hypertensive patients. HFrEF was indirectly caused by hypertension with IHD in younger age group and HFpEF was directly caused by hypertensive cardiomyopathy in older age group. Studies have identified various risk factors and pathogenic mechanisms for its development. In all studies, however, hypertension has emerged as a major risk factor.In practical terms, HFpEF is a clinical manifestation of hypertensive cardiomyopathy.The incidence and morbidity are similar to both HErEF and HFpEF. [8]
Proof of concept: Beneficial effects of BP lowering drugs-
Atrial Fibrillation
Atrial Fibrillation (AF) is common in hypertensive patients due to hypertensive cardiomyopathy and IHD. In a cohort of 4.3 million adults, an increase of 20 mmHg in systolic BP was associated with a 21% higher incidence of atrial fibrillation (relative risk (RR) 1.21, 95% confidence interval (CI) 1.19–1.22). Hypertension is one of the major score factor in CHADS2 and CHADS2VASd score of AF. [9]
Aortic stiffness and aortic syndrome
Hypertension is the predominant risk factor for development of aortic stiffness. On the other hand, aortic stiffness promotes rises in systolic and central BP in elderly individuals. Aortic syndromes—aneurysm and dissection—are in large part resultant from high BP. [10]
Aortic valve stenosis
Long-term exposure of the aortic valve leaflets to sustained blood flow at high pressure and arterial wave reflection due to aortic stiffness and increasing central BP lead to aortic valve calcification and aortic valve stenosis (AS). It is more common in bicuspid aortic valve. [11]
In a cohort of 101 patients with aortic stenosis evaluated by computed tomography, systolic hypertension was the strongest risk factor for progression of aortic valve calcification. High BP is the major risk factor for development of aortic stenosis in the elderly. [11]
Peripheral artery disease
In a cohort of 4.2 million adults, that an increase of 20 mmHg in usual systolic BP was associated with a 63% higher risk of peripheral arterial disease. The habit of smoking prevails as a risk factor. [12]
Chronic kidney disease
In Multiple Risk Factors Intervention Trial (MRFIT) cohort study, parallel increase between the risk of end stage renal disease and the stages of hypertension, but participants did not have their baseline kidney function assessed. In vice versa, hypertension was secondary to CKD. [13]
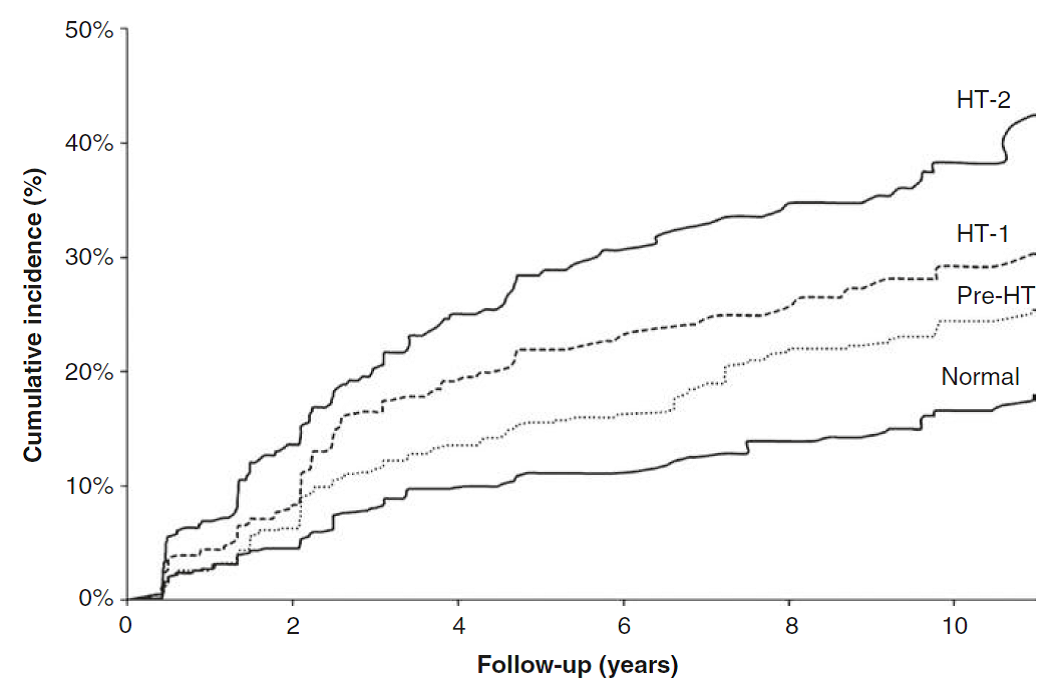
Fig: Cumulative incidence of CKD in hypertension, Prehypertension (Pre-HT),Stage 1 hypertension (HT-1), Stage 2 hypertension (HT-2) [13]
Dementias
Dementias are other consequences of high BP. Vascular dementia is more clearly associated with hypertension.A statement from the American Heart Association recognized BP in midlife as a strong risk factor for Alzheimer disease. [14]
Diabetes mellitus
Hypertension is a possible risk factor for development of Diabetes Mellitus. In a cohort study of 4.1 million adults who were free of diabetes at baseline, 20 mmHg higher systolic BP and 10 mmHg higher diastolic BP were associated with 58% and a 52% higher risks of new-onset diabetes, respectively. [15]
Age related macular degeneration
Age-related macular degeneration (AMD) is one of the leading causes of blindness in the elderly.The association between BP and AMD is controversial. [16]
Erectile dysfunction
Hypertension is a risk factor for erectile dysfunction. In a meta-analysis of 40 studies, including 121,641 individuals, hypertension was associated with a risk of 1.74 (95% CI 1.63–1.80) for the incidence of erectile dysfunction. [17]
References:
- Fruchs FD, et al. Essential of Hypertension: 120/80 paradigm. 1st edition. Springer International Publishing AG 2018
- O’Donnell MJ, Chin SL, Rangarajan S, et al. On behalf ofthe INTERSTROKE investigators. Global and regionaleffects of potentially modifiable risk factors associated withacute stroke in 32 countries (INTERSTROKE): a case-controlstudy. Lancet. 2016;388:761–775.
- Kjeldsen SE, Narkiewicz K, Burnier M, Oparil S, qt al. The INTERSTROKE Study: hypertension is by far the most importantmodifiable risk factor for stroke. Editorial. Blood Pressure. 2017; 26:3: 131-132.
- World Health Report 2002: Reducing risks, promoting healthy life. Geneva: World Health
Organization; 2002. - Law MR, Morris JK, Wald NJ, et al. Use of blood pressure loweringdrugs in in the prevention of cardiovascular disease:meta-analysis of 147 randomised trials in the context ofexpectations from prospective epidemiological studies. BMJ.2009;338:b1665.
- Baguet JP, Mallion JM, et al. Hypertension and coronary heart disease. European Society of Hypertension newsletter. 2005; 6; 14 r.
- Kuroda K, Kato TS, Amano A, et al. Hypertensive cardiomyopathy: A clinical approach and literature review. World J Hypertens. May 23, 2015; 5(2): 41-52.
- Redfield MM. Heart failure with preserved ejection fraction. N Engl J Med. 2016;375:1868–77.
- Emdin CA, Anderson SG, Salimi-Khorshidi G, Woodward M, MacMahon S, Dwyer T, et al.Usual blood pressure, atrial fibrillation and vascular risk: evidence from 4.3 million adults.Int J Epidemiol. 2017;46(1):162–72.
- Goldfinger JZ, Halperin JL, Marin ML, Stewart AS, Eagle KA, Fuster V. Thoracic aorticaneurysm and dissection. J Am CollCardiol. 2014;64(16):1725–39.
- Otto CM, Prendergast B. Aortic-valve stenosis—from patients at risk to severe valve obstruction.N Engl J Med. 2014;371:744–56.
- Emdin CA, Anderson SG, Callender T, Conrad N, Salimi-Khorshidi G, Mohseni H, et al.Usual blood pressure, peripheral arterial disease, and vascular risk: cohort study of 4.2 millionadults. BMJ. 2015;351:h4865.
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al. Blood pressureand end-stage renal disease in men. N Engl J Med. 1996;334(1):13–8.
- Iadecola C, Yaffe K, Biller J, Bratzke LC, Faraci FM, Gorelick PB, et al. Impact of hypertensionon cognitive function: a scientific statement from the American Heart Association.Hypertension. 2016;68(6):e67–94.
- Emdin CA, Anderson SG, Woodward M, Rahimi K. Usual blood pressure and risk of new-onsetdiabetes evidence from 4.1 million adults and a meta-analysis of prospective studies.J Am CollCardiol. 2015;66:1552–62.
- Katsia VK, Marketoub ME, Vrachatisc DA, Manolisd AJ, Nihoyannopoulosc P, Tousoulis D, et al. Essential hypertension in the pathogenesis of age-related macular degeneration: areview of the current evidence. J Hypertens. 2015;33:2382–8.
- Ning L, Yang L. Hypertension might be a risk factor for erectile dysfunction: a meta-analysis.Andrologia. 2017;49(4). https://doi.org/10.1111/and.12644.
Maung Maung Htay
MBBS, MMedSc(Int Med), MMed(NUS), MRCP(UK), MAcadMED(UK), Parami General Hospital


