Background
Esophageal manometry measures the different factors that play a role in the motility and function of the upper esophageal sphincter (UES), the body of the esophagus, and the lower esophageal sphincter (LES).
The esophagus can be affected by a variety of disorders that may be intrinsic or secondary to another pathologic process, but the resulting symptoms are usually not pathognomonic for a specific problem, making diagnosis somewhat challenging. Although detailed history taking, review of symptoms, and physical examination can orient the clinician in the right direction, further tests, including esophageal manometry, are sometimes necessary for establishing a diagnosis. The first attempts to test esophageal function date back to 1883, but the technology that would allow a proper recording of esophageal pressure dynamics was not developed until the 1970s.
Indications
- Evaluation of noncardiac chest pain or esophageal symptoms not diagnosed by endoscopy (or after gastroesophageal reflux disease [GERD] has been excluded)
- Evaluation for achalasia or another type of nonobstructive dysphagia
- Preoperative evaluation for patients undergoing corrective surgery for GERD, particularly if an alternative diagnosis like scleroderma or achalasia is being considered
- Postoperative evaluation of dysphagia in patients who underwent corrective surgery for reflux or after treatment of achalasia
- Prior to esophageal pH monitoring to assess the location of the LES for proper electrode positioning
- Evaluation of esophageal motility problems associated with systemic diseases
Contraindications
- Patients with altered mental status or obtundation
- Patients who cannot understand or follow instructions
- Suspicion or known pharyngeal or upper esophageal obstruction (eg, tumors)
Patient Preparation
Ideally, most patient should be instructed to fast for six hours, but this should be increased to twelve hours if achalasia is suspected because of the risk of aspiration given the possibility of food content in the esophageal lumen due to motor alterations.
Suspension of drugs that can alter esophageal motility on the day of the examination
This includes drugs such as calcium channel blockers, nitrates, prokinetics, loperamide, beta-receptor antagonists, opiates, and anticholinergics. These should only be used if suspension might lead to an alteration in the patient’s welfare.
Procedure
After catheter calibration and the application of a topical anesthetic to the patient’s naris and/or throat, the HRM catheter is placed transnasally and positioned with the pressure sensors spanning a length extending from the hypopharynx, through the esophagus, to 3 to 5 cm within the stomach. After a brief period to allow patient acclimation, a baseline of resting pressures can be obtained during approximately 30 seconds of easy breathing without swallows. Correct catheter placement to traverse the esophagogastric junction (EGJ) can be confirmed during this period by recognition of the presence of the pressure inversion point (PIP), which is the point at which the inspiration-associated negative intrathoracic pressure inverts to the positive intra-abdominal pressure. Having the patient take deep breaths facilitates identification of the PIP by augmenting the EGJ pressure and exaggerating the intrathoracic and intra-abdominal pressures. Once this measurement can be taken, the study continues with the patient taking ten swallows of 5 cc of water. It has recently been proposed that once ten swallows have been completed, multiple swallows should be added to the study to assess neuromuscular integrity. This is not yet standard, so implementation depends on the preference of the group conducting the study.
Chicago classification
The Chicago Classification for HRM creates a simplified and standardized way of analyzing the data from an HRM study to diagnose esophageal motility disorders. The three main measurements obtained by HRM that are used to make diagnoses are as follows:
- Integrated relaxation pressure (IRP)
- Distal latency (DL)
- Distal contractile integral (DCI)
The first decision point centers on evaluating the IRP as either normal (< 15 mm Hg) or abnormal (>15 mm Hg). Conditions with an abnormal IRP include the following
- Type I, II, and III achalasia
- EGJ outflow obstruction
- Major disorders of peristalsis – These include hypercontractile esophagus (jackhammer), distal esophageal spasm (DES), and absent contractility
- Minor disorders of peristalsis – These include fragmented peristalsis and ineffective esophageal motility (IEM)
- Normal motility
The Chicago Classification eliminates the diagnoses of hypertensive LES, nutcracker esophagus, hypotensive LES, and hypocontractile LES.
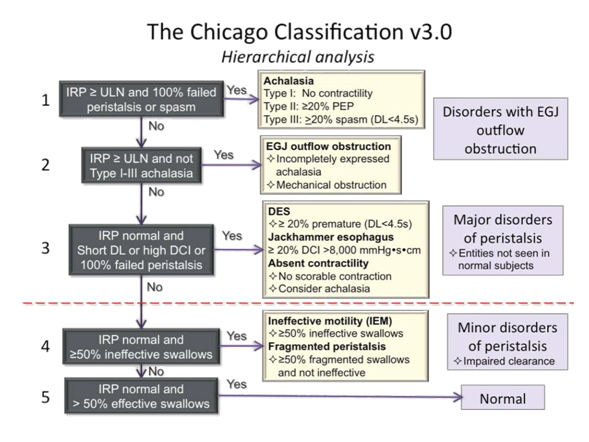
Fig 1: Hierarchical analysis of Chicago classification v3.0

Fig 2: Esophageal manometry machine and catheter
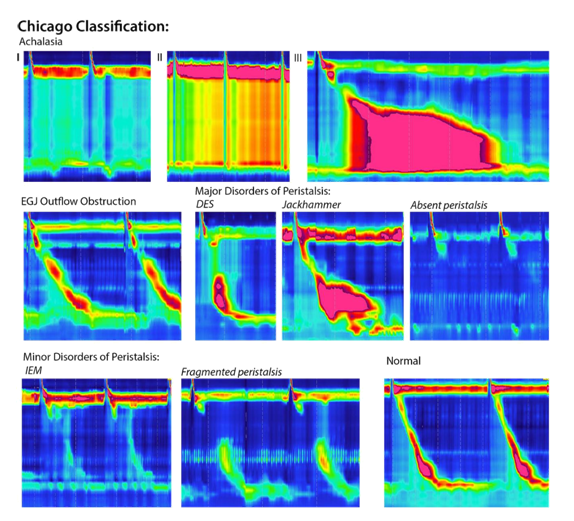
Fig 3 : Esophageal manometry plots
In this figure, examples of high manometry color plots are shown of the individual disorders as classified in the Chicago classification. Distal esophageal spasm (DES), Ineffective esophageal motility (IEM), Esophagogastric junction (EGJ).
Complications
Esophageal manometry is a generally safe procedure, and complications are usually few and mild (e.g., gagging and watery eyes during the catheter insertion, sore throat, rhinorrhea, and epistaxis). More severe complications occur rarely and may include arrhythmias, vasovagal episodes, bronchospasm, and aspiration .In situations where manometry must be performed despite the presence of relative contraindications, precautions such as endoscopic or radiologic guidance must be performed to decrease the risk of complications.
The following charts show number of patients, in month, who have undergone esophageal manometry at Department of Gastroenterology, Yangon General hospital from 2015 to July 2018.
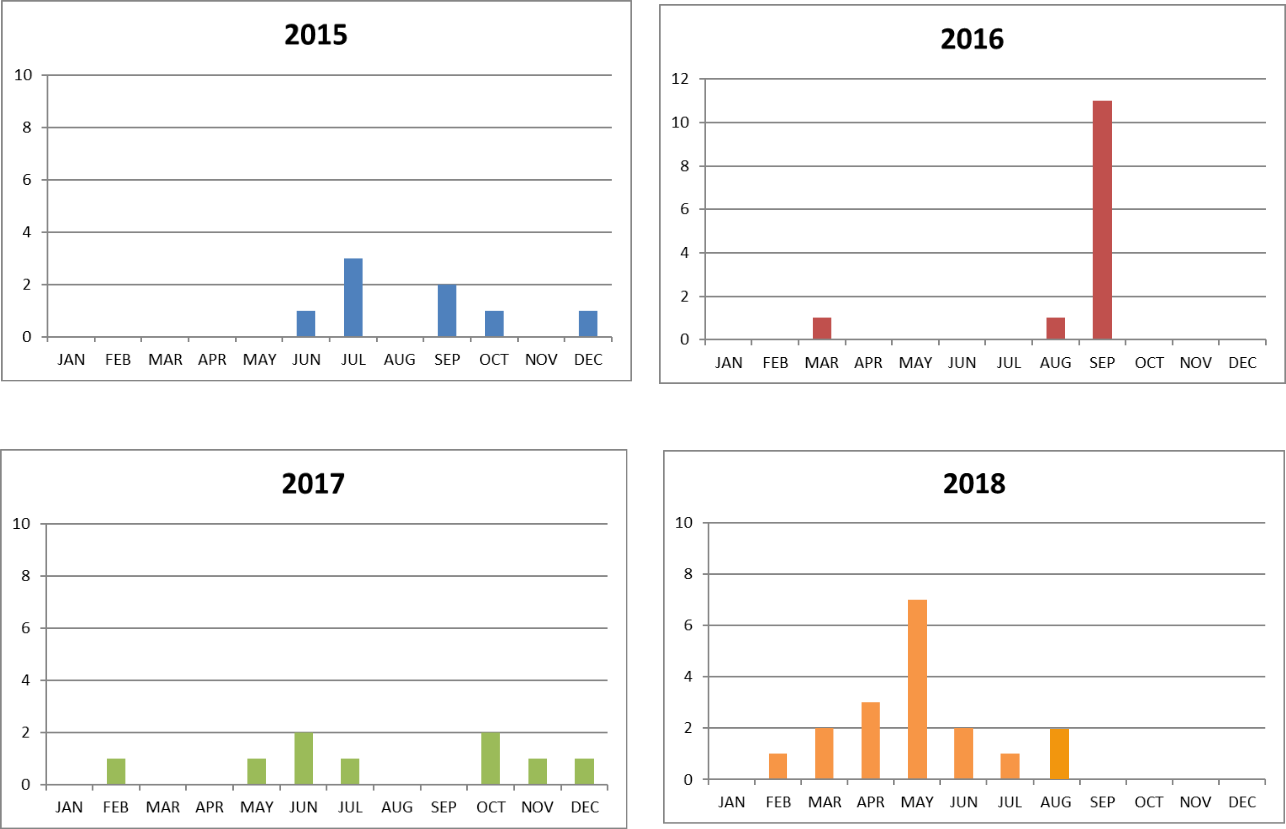
Fig 4: Number of patients who have undergone esophageal manometry at Department of Gastroenterology, Yangon General hospital, since 2015.
Thein Myint 1, Moe Myint Aung2, Tin Moe Wai 3, Swe Mon Mya4, Mya Thet Nwe4, Sandar Win4, Thida Soe4, Su Su Hlaing5
- Professor and Head, Department of Gastroenterology, Yangon General Hospital
- Professor, Department of Gastroenterology, Yangon General Hospital
- Associate Professor, Department of Gastroenterology, Yangon General Hospital
- Consultant Gastroenterologist, Department of Gastroenterology, Yangon General Hospital
- Doctorate student, Department of Gastroenterology, University of Medicine 1, Yangon
References
Rohof, W. O. A. & Bredenoord, A. J. (2017) Chicago Classification of Esophageal Motility Disorders:
Lessons Learned .Curr Gastroenterol Rep . 19(8), 37.
Hani, A., Leguízamo, A. M., Carvajal, J.J., Mosquera-Klinger, G. & Costa, V. A. (2015) How to Perform and Interpret High-resolution Esophageal Manometry, Rev Col Gastroenterol. 30(1), 68-74.
Kahrilas, P.J., Bredenoord, A.J., Fox, M., Gyawali, C.P., Roman, S., Smout, A.J. & Pandolfino, J.E. International High Resolution Manometry Working Group (2015) The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil. 27(2),160-174.
Katz, P.O., Sloan, J. & Rodrijuez, M.D.G. (2018) Esophageal manometry. Medscape.
https://emedicine.medscape.com/article/1891791. [Accessed on : 30th August 2018]