
Introduction
Dengue is a febrile illness caused by infection with one of four dengue viruses (DENV) transmitted by Aedesaegypti or Aedesalbopictus mosquitoes during the taking of a blood meal. Infection may be asymptomatic or present with a broad range of clinical manifestations including a mild febrile illness to a life-threatening shock syndrome (1)
Clinical Manifestations
Dengue virus infection may be asymptomatic or may cause undifferentiated febrile illness (viral syndrome), dengue fever (DF), or dengue haemorrhagic fever (DHF) including dengue shock syndrome (DSS). Infection with one dengue serotype gives lifelong immunity to that particular serotype, but there is only short-term cross-protection for the other serotypes. The clinical manifestation depends on the virus strain and host factors such as age, immune status.
Undifferentiated Fever
Those who have been infected with dengue virus, especially for the first time (i.e. primary dengue infection), may develop a simple fever indistinguishable from other viral infections (2).
Dengue fever (DF)
Clinical criteria that define DF include a 2-7 day illness with high fever, headache, retro-orbital pain, myalgia, arthralgia/bone pain, rash and haemorrhagic manifestations (positive tourniquet test or petechiae) with no evidence of plasma leakage(2).
Dengue Haemorrhagic Fever (DHF)
In the first few days DHF patients will have signs and symptoms similar to that of DF. However,they will develop features of plasma leakage later ( usually beyond day 3) The following criteria are necessary for the case definition of DHF
1. High fever or recent history of acute fever
2. Haemorrhagic manifestaions ( at least a positive tourniquet test)
3. Thrombocytopenia of ≤ 100, 000 cell/mm3
4. objective evidence of plasma leakage
N.B. In patients who have definite evidence of plasma leakage, presenceof haemorrhagic manifestation is not essential for the diagnosis of DHF(2).
Expended Dengue Syndrome (EDS)
Unusual manifestations of patients with severe organ involvement such as liver, kidneys, brain or heart associated with dengue infection have been increasingly reported in DHF and also in dengue patients who do not have evidence of plasma leakage. These unusual manifestations may be associated with coinfections, comorbidities or complications of prolonged shock. Exhaustive investigations should be done in these cases. Most of these unusual manifestations are the result of prolonged shock with organ failure or due to comorbidities or coinfections.
Phases of DHF /DSS
Febrile phase
Patients typically develop a high-grade fever suddenly. This acute febrile phase usually lasts 2−7 days which may be biphasic and is often accompanied by facial flushing, skin erythema, generalized body ache, myalgia, arthralgia, retro-orbital eye pain, photophobia, rubeliform exanthema and headache. Some patients may have a sore throat, an injected pharynx, and conjunctival injection. Anorexia, nausea and vomiting are common (3).
Critical phase
During the transition from the febrile to afebrile phase, patients without an increase in capillary permeability will improve without going through the critical phase. Instead of improving with the subsidence of high fever; patients with increased capillary permeability may manifest with the warning signs, mostly as a result of plasma leakage. The warning signs mark the beginning of the critical phase. These patients become worse around the time of defervescence, when the temperature drops to 37.5−38°C or less and remains below this level, usually on days 3–8 of illness. The period of clinically significant plasma leakage usually lasts 24−48 hours. If shock occurs when a critical volume of plasma is lost through leakage, it is often preceded by warning signs. The body temperature may be subnormal when shock occurs. With profound and/or prolonged shock, hypoperfusion results in metabolic acidosis, progressive organ impairment, and disseminated intravascular coagulation.
It may take a few hours for patients to progress from warning signs to compensated shock and another few hours for compensated shock to progress to hypotensive shock, but only minutes for hypotensive shock to progress to cardiorespiratory collapse and cardiac arrest(3).
Recovery phase
As the patient survives the 24−48 hour critical phase, a gradual reabsorption of extravascular compartment fluid takes place in the following 48−72 hours. General wellbeing improves, appetite returns, gastrointestinal symptoms abate, haemodynamic status stabilizes, and diuresis ensues. Some patients have a confluent erythematous or petechial rash with small areas of normal skin, described as “isles of white in the sea of red” (10).Some may experience generalized pruritus. Bradycardia and electrocardiographic changes are common during this stage (3).
Medical complications seen in the febrile, critical and recovery phases of dengue
Febrile phase : dehydration, febrile seizure
Critical phase : shock from plasma leakage, severe haemorrhage, organ impairment
Recovery phase : hypervolaemia and acute pulmonary oedema (3)
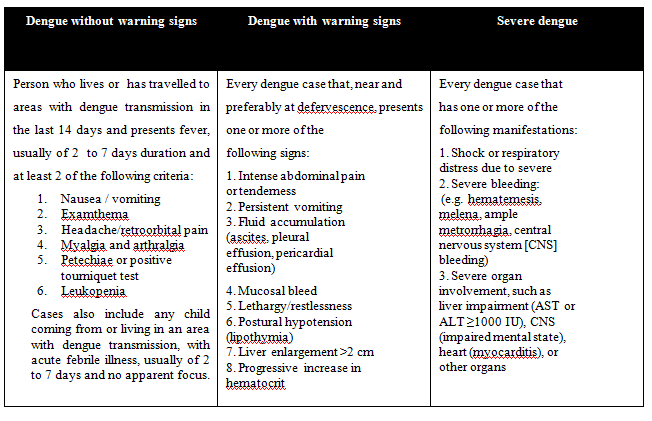
Modified dengue severity classification WHO 2009 (3)
Laboratory Investigations
The following figure demonstrate the virological and serological markers in relation to time of dengue infection
Virological and serological markers in relation to time of dengue infection (5)
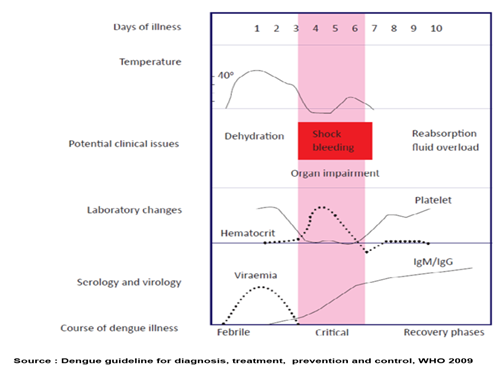
Course of dengue fever (4)
Febrile phase (day 1 to day 4–5 of fever)
The infective virus can be isolated in serum by tissue culture or using reverse transcriptase polymerase chain reaction (RT-PCR)
NS1 Ag is a marker of acute dengue infection. Both enzyme-linked immunosorbentassay (ELISA) and rapid commercial tests are available for NS1 Ag detection. The highest percentage of positive test on the first 2 days of fever (sensitivity 40-70%). On day four of fever, the percentage of positive test may be reduced to 30-40%.(6)
Critical and convalescent phases (after days 4–5 of illness)
Specific IgM is the best marker of a recent dengue infection. Primary infections are characterized by high levels of IgM and low levels of IgG, while low levels of IgM with high levels of IgG characterize secondary infections.
A single serum sample collected after day 5 of fever onset is useful for IgM determination Sensitivity for IgG/IgM is 60-80% on day of shock or defervescence and reached 100% on day after shock/defervescence.
Duo test (NS1Ag + IgM/IgG) is recommended between day 4 onwards , the overall sensitivity may increase to > 90%(5).
Laboratory warning sign of dengue
Leucopenia : occurs 24 hours before rapid decrease in platelet count
Thrombocytopeinia and rising trend in haematocrit:
Shortly before or at defervescence, may precede change in blood pressure and pulse pressure (5)
Management of Dengue
Stepwise approach to the management of dengue patients
Step 1: Overall assessment
Overall assessments include taking proper history, physical examination and laboratory investigations to get the clinical diagnosis of dengue and to exclude other differential diagnosis. Fever with a potential dengue diagnosis should get the following laboratory tests except in cases with uncommon manifestations (2).
Step 2: Diagnosis and assessment of disease phase and severity
To determine the phase, warning signs, and haemodynamic status and whether the patient requires hospital admission based on the anamnesis, physical examination, and laboratory results (2).
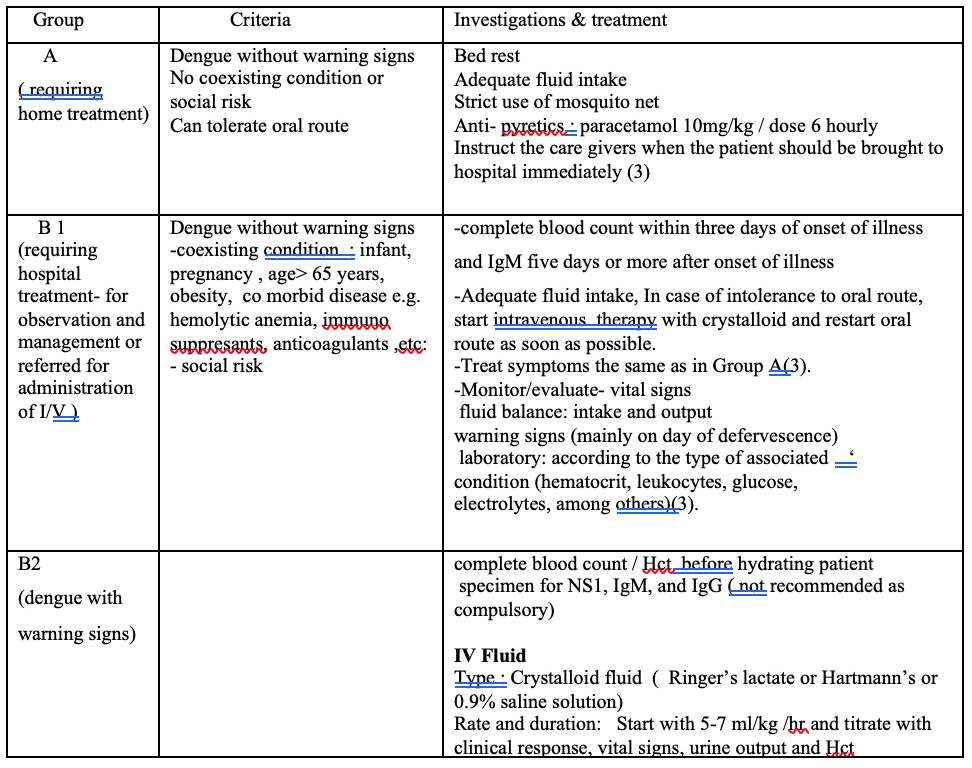
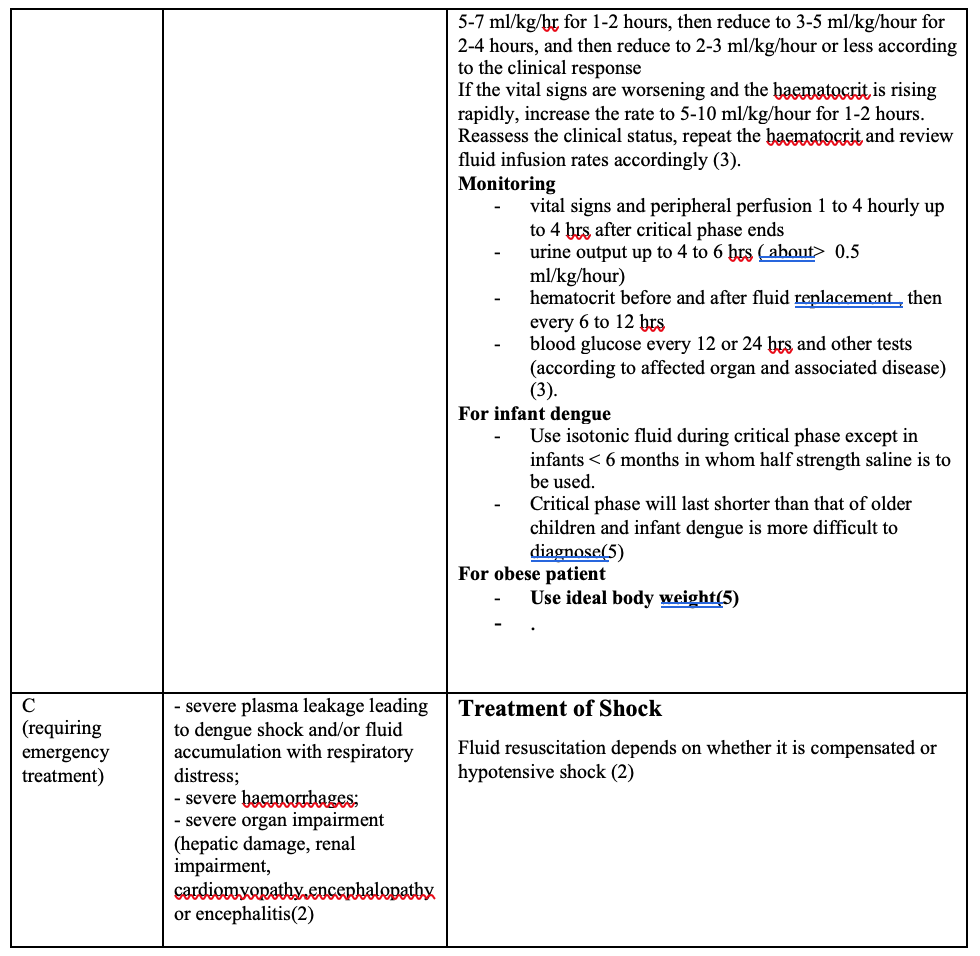
Step 3: Treatment
There are three groups according to clinical manifestations and circumstances
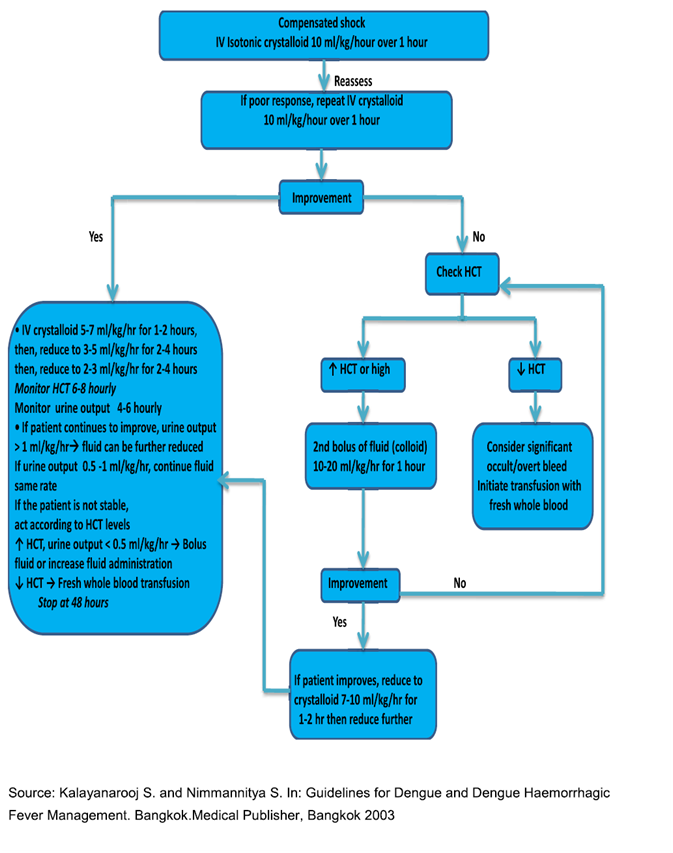
Algorithm for fluid management in compensated shock (2,7)
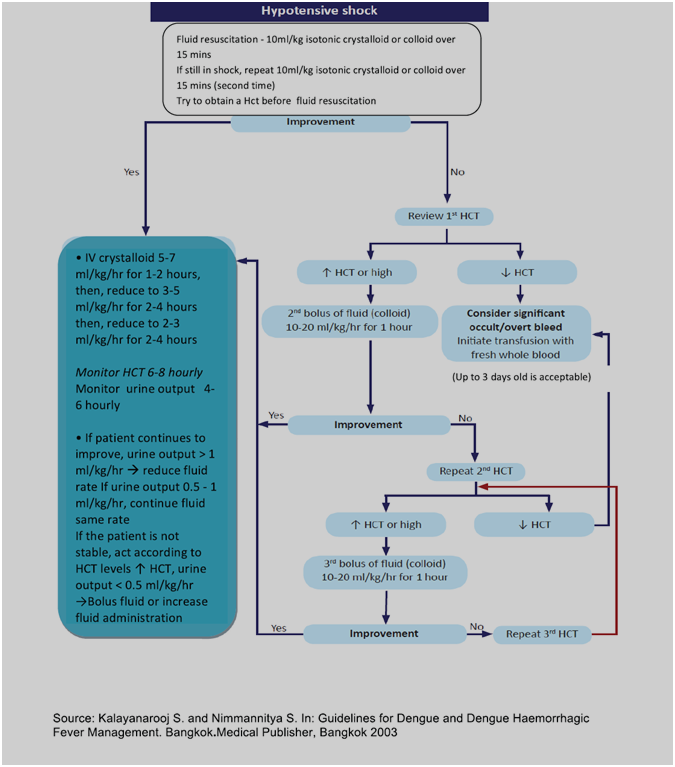
Algorithm for fluid management in hypotensive shock (2,7)
Treatment of haemorrhagic complications
The action plan for the treatment of haemorrhagic complications is as follows:
- If possible, stop bleeding if the source of bleeding is known.
- give 5-10 ml/kg of fresh -packed red cells or 10-20 ml/kg of fresh or fairly fresh whole blood (Consider repeating the blood transfusion if there is further overt blood loss or no appropriate rise in haematocrit
- no evidence to support for transfusing platelet concentrates and/or fresh-frozen plasma for severe bleeding in dengue
- It is being practices when massive bleeding cannot be managed with just fresh whole blood/ fresh-packed cells (but it may exacerbate the fluid overload)(2).
Discharge criteriaies B1
All these criteria should be met at the same time:
–– absence of fever for 48 hours, without administration of antipyretics
–– improvement of clinical status
- general well-being
- good appetite
- normal hemodynamic status
- normal or increased urine output
- no respiratory distress
- no evidence of bleeding
–– increasing trend for platelet count
–– stable hematocrit without administration of IV fluid (3)
Pearls and Pitfalls in the management of dengue
The clinical management of dengue is more fraught with pitfalls than that of most other infectious tropical diseases (5).
Pitfall 1: Recognition of dengue at the frontline
The frontline physician does not recognize dengue when the patient presents as a febrile illness in the first few days, and no follow-up is given.
Pearls 1: The only way to recognize dengue in the early febrile phase is to suspect it in every febrile patient. If the patient fulfils the criteria for probable dengue, the physician should inform the patient about the suspected disease and schedule daily follow-up and advice with immediate medical attention if warning signs occur.
Pitfall 2: Missed opportunity for FBC in early febrile period
Full blood count (FBC) not determined until day 4 of illness.
Pearls 2: A full blood count should be done at the first visit when dengue is suspected.
Pitfall 3: Not understanding the evolving FBC
Full blood count is “normal” and the physician excludes the diagnosis of dengue.
Pearls 3: The early and progressive decrease in white cell and platelet counts during the febrile period is a useful indicator of dengue.
Pitfall 4: Waiting for full blood count results (for thrombocytopenia)
Waiting for FBC results to make decisions about admission and intravenous fluid therapy will cause further delay in recognition and treatment of dengue shock.
Pearls 4: Intravenous fluid therapy should be initiated when warning signs or clinical evidence of shock are present.
Pitfall 5: Vital signs are “stable”
This phrase means that the patient is alert and has BP within the normal range. These two conditions are present in compensated shock. The patient in shock remains in this quiet alert state until cerebral perfusion diminishes, and then develops a “sudden” shortness of breath and restlessness or seizures followed quickly by a “sudden” collapse.
Pearls 5: assess the peripheral perfusion of every patient, not only dengue patients. It takes less than 30 seconds to assess the four parameters: pulse volume, capillary refill time, colour and temperature of the extremities.
Pitfall 6: Symptomatic treatment with antispasmodic agents or antacid is being given to patients with abdominal pain or they are referred to the surgical team or for ultrasound studies.
Abdominal pain is an early sign of plasma leakage and becomes more severe as hypovolaemia progresses.
Pearls 6: A history of transitioning from fever to no-fever and the development of gastrointestinal symptoms such as nausea, vomiting or diarrhoea, should suggest dengue with warning signs or dengue shock.
Pitfall 7: Bleeding versus plasma leakage
The physician, who is overly concerned about the risks of bleeding, focuses on monitoring the trend of platelet counts alone to the exclusion of the bigger picture of plasma leakage. These physicians may administer platelet transfusions in addition to the maintenance of intravenous fluid. Fluid overload or inadequate fluid replacement may ensue, depending on the severity of the plasma leakage and the phase of disease at the time of platelet transfusion. Inadequate fluid replacement leads to prolonged and profound shock characterized by bleeding, the very phenomenon that these physicians are trying to prevent. It is important to note that the platelet count may remain low/very low during the first one or two days of recovery and that platelet transfusion during this time will cause fluid overload (7).
Pearls 7: The physician should be alert to the onset of this unique syndrome of dengue vasculopathy that causes plasma leakage and hypovolaemic shock when the fever subsides. Monitoring should be focused on manifestations of plasma leakage, bleeding and shock. The trend of haematocrit level together with haemodynamic status is the main guide to fluid management.
The usefulness of trending of the platelet count during the febrile phase is to identify its rapid decrease, which marks the beginning of plasma leakage. Beyond this phase, trending of platelet counts has no bearing on fluid management.
Pitfall 8: Starting intravenous fluids in the febrile phase (because NS1 Ag ispositive)
This practice should not be routine. Early intravenous fluid therapy will exacerbate accumulation of third space losses before the critical phase when plasma leakage increases significantly.
Pearls 8: During the febrile phase hydration should be maintained by the oral route .Only in exceptional cases should intravenous infusion be used and then it should be kept at a minimal infusion rate and be discontinued as soon as the patient can take oral fluids.
Pitfall 9: Increased fluid therapy in a well perfused patient with persistently elevated haematocrit.
The haematocrit may remain elevated towards the end of the critical phase (24−48 hours of plasma leakage) despite adequate fluid therapy. An attempt to correct the haematocrit level by increasing intravenous fluid therapy will often lead to fluid overload.
Pearls 9: Continue close monitoring. Do not increase the intravenous fluid therapy; if the patient continues to be well perfused.
Pitfall 10: During the critical phase the urine output of 1 ml/kg/hour is used as a criterion of adequate intravenous therapy or might not be monitored at all.
During the critical phase the urine output is a useful indicator of the intravascular volume state but should not be used as the sole criterion.
Pearls 10: In severe shock, urine output should be monitored hourly using an indwelling catheter. The expectation of what constitutes an adequate urine output should be scaled down to ~ 0.5 ml/kg/hour to avoid fluid overload. On the other hand, a urine output exceeding that may be an indication to reduce intravenous fluid therapy.
Pitfall 11: Worsening or persistent abdominal pain/tenderness appearing after 24 hours of large volumes of fluid replacement, misinterpreted as “warning sign for shock”.
After more than 24 hours’ administration of large volumes of fluid, tense ascites would have developed in patients with severe plasma leakage. These patients often complain of abdominal discomfort or pain. This may be due to tense ascites and/or enlarged and congested liver from the fluid overload.
Pearls 11: This symptom and sign should be interpreted cautiously. Intravenous fluid should be changed to colloids or be reduced and discontinued. Further fluid replacement will not only increase the abdominal symptoms but also aggravate the respiratory distress.
Pitfall 12: Not transfusing blood until the haematocrit has decreased to low levels in unstable patients.
Severe but occult bleeding can be difficult to recognize.
The haematocrit will only decrease to low levels after several boluses of fluid resuscitation (especially with colloids), or if the bleeding has been very severe. Throughout the period of fluid resuscitation the patient remains unstable while the “third space” fluid accumulation increases.
Pearls 12: It is critical to recognize that the lower the haematocrit in dengue shock the more likely the significant bleeding, and therefore it is vital to change strategy from crystalloid/colloid infusion to blood transfusion.
Pitfall 13: Blood transfusion in a stable patient with low haematocrit.
This usually occurs during the recovery period when re-absorption causes haemodilution. A blood transfusion at this stage may precipitate life-threatening pulmonary oedema.
Pearls 13: If the patient has a stable circulation they do not need blood transfusion. The haematocrit will increase after the excess fluid has been diuresed.
Pitfall 14: Last but not least, dengue shock treated “aggressively” as in septic shock
The strategy of aggressive fluid resuscitation of septic shock is not applicable to severe dengue with plasma leakage. Aggressive fluid resuscitation may indeed be harmful and should be limited to dengue shock with hypotension.
Pearls 14: Once the peripheral pulses are established the rate of parenteral fluid replacement should be reduced, as per frequent and simultaneous haemodynamic and haematocrit assessment.
References
Up To Date [Internet]. Uptodate.com. 2020 [cited 29 April 2020]. Available from: Monitor/evaluate
–– vital signs
–– fluid balance: intake and output
–– warning signs (mainly on day of defervescence)
–– laboratory: according to the type of associated condition (hematocrit, leukocytes, glucose, electrolytes, among others)(3).
- Vector Borne Disease Control Programme. National Guideline for Clinical Management oF Dengue. 1st ed. Myanmar: Ministry of Health and Sports; 2017.
- Pan American Health Organization. Dengue: guidelines for patient care in the Region of the Americas. 2nd ed. Washington: Pan American Health Organization; 2016
- World Health Organization. Dengue: guidelines for diagnosis, treatment, prevention and control. 1st ed. Geneva: World Health Organization; 2009.
- World Health Organization. Handbook for clinical management of dengue. Geneva: World Health Organization; 2012
- Kalayanarooj S. Clinical Manifestations and Management of Dengue/DHF/DSS. Tropical Medicine and Health. 2011;39(4SUPPLEMENT):S83-S87
- Kalayanarooj, Nimmannitya. Guidelines for dengue and dengue haemorrhagic fever management. Bangkok: Bangkok Medical Publisher; 2004
Authour information
@Saw Win. MBBS, DCH, MMedSc (Paed.), MRCP, MRCPCH, FRCPE,DCH(Glas.),DTM&H (Lond.),Dip Med Ed. Consultant paediatrician, Parami and Bahosi Hospital
*Kyi San Thi. MBBS, MMedSc (Paed.),MRCPCH. Specialist Medical Officer (Paediatrics) , Yankin Children Hospital
