Changing Perceptions
From the Stone Age to the Renaissance, fatness or obesity was viewed as beautiful, healthy, and a sign of prosperity 1. This concept prevailed with famines and wars, and fatness was viewed as a guarantee against starvation. Worldwide, socially dominant groups (the rulers and the prosperous) with better access to resources, such as food and the new smallpox vaccine were believed to have better nutrition and health. Fat women were considered testimony to their husbands’ wealth. At the turn of the 20th century, actress Lillian Russell — tipping the scale at 200 pounds — was a reigning sex symbol, with her photos displayed in many newspapers.

With the advent of motor vehicles, levels of physical activity declined. Food becoming more abundant also exacerbated the unhealthy effects of being obese, raising public awareness. By 1900, there was a slight movement to diet or lose weight. “An excess of flesh is to be looked upon as one of the most objectionable forms of disease.”
The boyish look became popular in the USA in the 1920s, and being thin became an increasingly popular body image. Models like Twiggy in the 1970s further promoted thinness as beauty. By the 1980s, as AIDS loomed on the horizon, a fuller body became more desirable.
Over the years, evidence of the link between obesity and non- communicable diseases accumulated, and obesity is no longer a merely cosmetic concern but has emerged as a global health problem.
What is Obesity?
The World Health Organization defines obesity according to body mass index (weight in kilograms divided by height in meters squared). BMI provides the most useful population-level measure of overweight and obesity as it is the same for both sexes and for all ages of adults. However, it should be considered a rough guide because it may not correspond to the same degree of fatness in different individuals. For children, age needs to be considered when defining overweight and obesity2
For adults, the WHO defines overweight and obesity as follows:
- overweight is a BMI greater than or equal to 25; and
- obesity is a BMI greater than or equal to 30.
For children under 5 years (WHO child growth standards for children aged under 5 years)
- overweight is weight-for-height greater than 2 standard deviations above WHO Child Growth Standards median
- obesity is weight-for-height greater than 3 standard deviations above the WHO Child Growth Standards median.
For children aged between 5–19 years (WHO child growth standards for children aged under 5 years)
- overweight is BMI-for-age greater than 1 standard deviation above the WHO Growth Reference median; and
- obesity is greater than 2 standard deviations above the WHO Growth Reference median.
Raised BMI is a major risk factor for non-communicable diseases such as:
- cardiovascular diseases (mainly heart disease and stroke), the leading causes of death in 2012;
- diabetes
- musculoskeletal disorders (especially osteoarthritis- a highly disabling degenerative disease of the joints);
- some cancers (including endometrial, breast, ovarian, prostate, liver, gallbladder, kidney, and colon).
The risk for these non-communicable diseases increases, with increases in BMI.
Conceptually, obesity can be defined as a level of body weight and adiposity that is sufficiently excessive to damage health, demonstrated by an increased risk of various chronic diseases3.
Theories of pathogenesis
- Genes – Genes can directly cause obesity in disorders such as Bardet-Biedl syndrome and Prader-Willi syndrome. However, both genes and behaviour may be needed to result in obesity; and multiple genes may increase the susceptibility. It is now well established that overweight and the different forms of obesity tend to concentrate within a family. Obesity risk is two to eight times higher for a person with a family history as opposed to a person without history. Heritability of obesity may vary depending on the phenotype and rates tend to be higher for phenotypes linked to adipose tissue distribution (40-55%) and for weight or body fat excess (5-40%). Weight gain and adiposity increase with age, an effect also influenced by heredity4.
- Imbalance between calories consumed and calories expended. Globally, there has been an increased intake of energy-dense foods that are high in fat; and an increase in physical inactivity due to the increasingly sedentary nature of many forms of work, changing modes of transportation, and increasing urbanization2.
- Obesogenic environments– The combination of insulinogenic diets and psychosocial stress on the one hand, and low energy demand for physical exertion, reproduction and immune function on the other, stimulates chronic lipogenesis but reduces lipolysis. We are changing from a species that is well adapted to diverse ecological niches into a species in which a large proportion of individuals are characterized by excess body weight that impacts adversely on health 5
- Metabolic efficiency- individuals belonging to different ethnic groups differ in metabolic efficiency; those with lower energy expenditure while maintaining the same body weight are more efficient and therefore more prone to weight gain6
- Homeostatic imbalance in the psychological sphere. If, for whatever reason, high levels of dissatisfaction, negative affect, consumption or increased body weight should arise, then the interactivity through the feedback loops forms a vicious circle, a disturbance to the stability of the system that controls weight gain7
- Imbalance of energy homeostasis- orexigenic hormones stimulate feeding and may induce hyperphagia e.g. ghrelin, orexin or neuropeptide Y. Anti-orexigenic hormones e.g. leptin which is produced by adipose tissue is an appetite depressant. The levels normally rise during sleep, subduing the need to eat by “reassuring” the brain that energy reserves are adequate for the time being. Hypothalamic obesity(HO) results from lesions in the ventromedial nucleus and paraventricular nucleus, resulting in resistance to anti-orexigenic hormones
Energy homeostasis
This is a relatively recent term. Feeding is one of three “appetitive behaviours” (the other two are sleep and sex) and is influenced mainly by biological factors in most animals. In humans societal and psychological factors have important roles.
The classical theory of regulation of food intake is a simple model of two centers in the hypothalamus: the “satiety centre” located in the paraventricular nucleus (PVN) and spontaneously active “feeding center” in the lateral hypothalamus. The PVN is stimulated by an increase in arteriovenous difference in blood glucose level and inhibits the feeding center. The hyperphagia of uncontrolled diabetes is due to the low (A-V) difference in blood glucose. External influences like psychological factors, food availability, social interactions were not given much thought. As students, we were familiar with the picture of the obese rat with a lesion in the PVN compared with its normal litter mate. The details of why obesity results were not known then.
The advances in knowledge in recent years have now been consolidated to present a more complicated picture. Many nuclei in the hypothalamus as well as the superchiasmatic nuclei are involved, together with insulin, intestinal hormones, signals from the gut ( gut-brain axis), and hormones produced by adipose tissue ((leptin, asprosin). Hypoglycemic hormones e.g. insulin, IGF-1 and hyperglycaemic hormones like glucagon, catecholamines also take part in regulating food intake through regulating blood glucose levels. Other factors like type of fat distribution 8, sleep deprivation 9 also have important roles in the genesis of obesity.
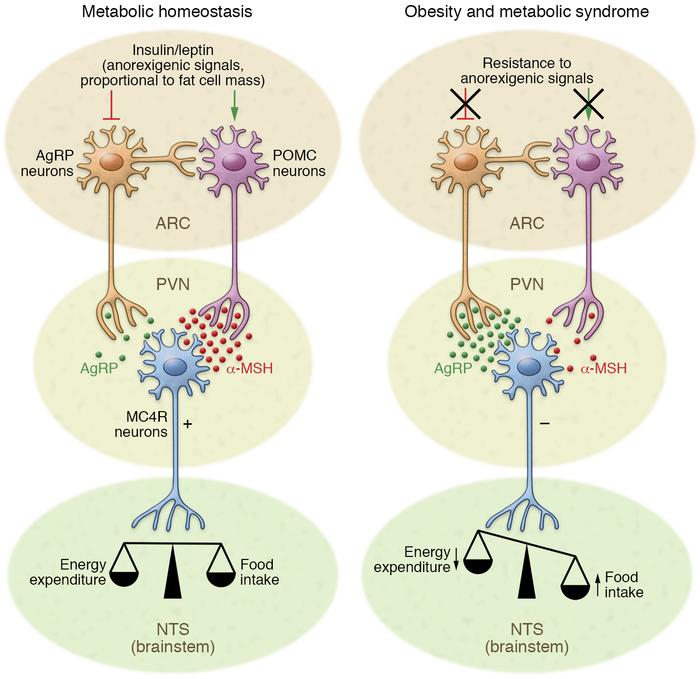
Source- Jais A &Bruning J J Clin Invest. 2017;127(1):24-32
1. Hypothalamic nuclei involved
- Arcuate nucleus (ARC)- produces orexigenic peptides, neuropeptide Y, opioids, dynorphin, POMC-derived peptide, β endorphin, galandin, amino acids, gamma amino butyric acid, glutamate
- Ventromedial and lateral hypothalamus – containing the “satiety center”
- Dorsomedial nuclei- responds to orexigenic signals (feeding)
- Paraventricular nucleus (PVN) and perifornical nuclei- ingestive behaviour
(feeding as a result of orexigenic signals and reducing food intake with anti-orexigenic /
anorexigenic signals).
Insulin and leptin act directly on neuronal subsets in the ARC of the hypothalamus to control energy homeostasis. Through activation of POMC neurons and inhibition of AgRP neurons, adipostatic signals activate MC4R-expressing neurons in the PVN. During fasting conditions, the expression of AgRP increases, whereas POMC expression is reduced, resulting in decreased MC4R signalling. In the fed state, AgRP levels are diminished and POMC levels increase, which triggers MC4R signalling and culminates in satiety and stimulation of energy expenditure. Neuronal inflammation and the subsequent insulin and leptin resistance of ARC neurons disrupts this metabolic feedback loop, further promoting increased food intake and body weight gain10. - Superchiasmatic nucleus- circadian pattern of feeding , influenced by light-dark cycles
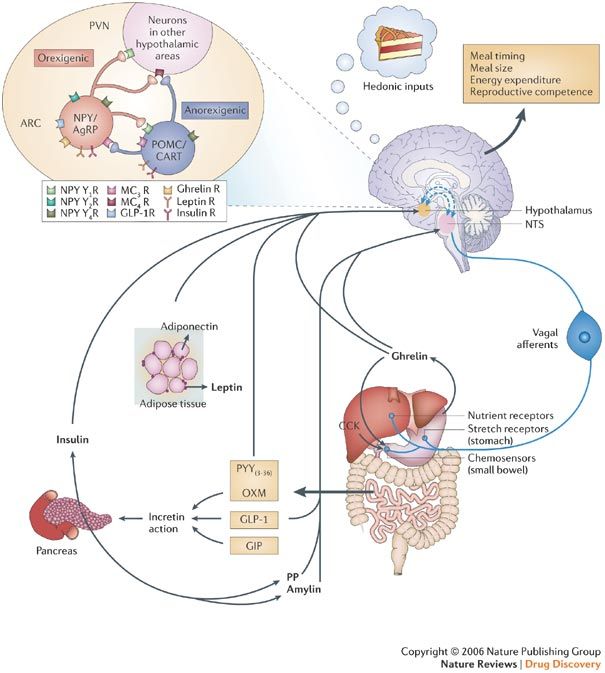
2. Hormonal influences
Orexigenic hormones (orexin, ghrelin, neuropeptide Y) act on hypothalamic nuclei to stimulate feeding whilst anorexigenic hormones (insulin, leptin) inhibit feeding. Resistance to the latter leads to development of the Metabolic syndrome.
3. Gut-brain axis
Vagal afferents from the gut carry signals from stretch, nutrient and chemoreceptors from the gut 11 to the hypothalamic nuclei “informing” the brain about the energy status (particularly of carbohydrate; less of fat) and also bring on the sensations of hunger or fullness.
4. Eating disorders12
Eating disorders are now officially recognized as mental disorders by the Diagnostic and Statistical Manual of Mental Disorders (DSM).Individuals with eating disorders can have a variety of symptoms but most include the severe restriction of food, food binges or inappropriate purging behaviours like vomiting or over-exercising. Although eating disorders can affect people of any gender at any life stage, they are most often reported in adolescents and young women.
(1) Anorexia nervosa is likely the most well-known eating disorder. It generally develops during adolescence or young adulthood and tends to affect more women than men. Affected people avoid eating. (Karen Carpenter of “Top of the World” fame died from this).
(2) Bulimia also tends to develop during adolescence and early adulthood and appears to be less common among men than women. They tend to eat until full and induce vomiting (The Princess of Wales suffered from this malady).
(3) Binge eating typically begins during adolescence and early adulthood, although it can also develop later and is characterised by: eating large amounts of foods rapidly; in secret and until uncomfortably full, despite not feeling hungry; and then feeling ashamed.
(4) Pica can occur in adults, as well as children and adolescents but is most frequently observed in children, pregnant women and individuals with mental disabilities. It manifests as a craving for non-food substances such as ice, dirt, soil, chalk, soap, paper, hair, cloth, wool, pebbles, and laundry detergent.
(5) Rumination disorder a person regurgitates food they have previously chewed and swallowed, re-chews it and then either re-swallows it or spits it out; this typically occurring within the first 30 minutes after a meal. Unlike medical conditions such as reflux, it is voluntary.
(6) Avoidant or restrictive food intake disorder (ARFID) is what was known as a “feeding disorder of infancy and early childhood,” a diagnosis previously reserved for children under seven years old. Although ARFID generally develops during infancy or early childhood, it can persist into adulthood. What’s more, it is equally common in men and women. Individuals with this disorder experience disturbed eating either due to a lack of interest in eating or a distaste for certain smells, tastes, colours, textures or temperatures.
Medical conditions presenting as obesity
Obesity is not always a result of imbalance between energy intake and expenditure but may be a manifestation of a disease. These may be due to metabolic imbalance such as :Metabolic Syndrome (increased blood pressure, hyperglycaemia, visceral obesity, low HDL , and raised cholesterol or triglyceride levels); Syndrome X(high intake of refined carbohydrates, leading to hypoglycaemia, hyperinsulinemia, and glucose intolerance followed by diminished insulin sensitivity, further leading to hypertension, hypercholesterolemia, obesity, and T2DM); hormonal imbalance such as Cushing’s Syndrome, Polycystic Ovarian Syndrome and hypothyroidism13 ; or neural cause as in hypothalamic obesity.
Prevention of Obesity
Prevention and treatment of obesity has focused on pharmacological, educational and behavioural interventions, with limited overall success. A novel and a longer-term approach would be to investigate the environments (Obesogenic environments) that promote high energy intake and sedentary behaviour 14, 15. The obesogenicity of an environment has been defined as “the sum of influences that the surroundings, opportunities, or conditions of life have on promoting obesity in individuals or populations”.
The WHO Response2
Adopted by the World Health Assembly in 2004, the “WHO Global Strategy on Diet, Physical Activity and Health” describes the actions needed to support healthy diets and regular physical activity. The Political Declaration of the High Level Meeting of the United Nations General Assembly on the Prevention and Control of Non-communicable Diseases of September 2011, recognizes the critical importance of reducing unhealthy diet and physical inactivity. At the individual level, people can:
- limit energy intake from total fats and sugars;
- increase consumption of fruit and vegetables, as well as legumes, whole grains and nuts; and
- engage in regular physical activity (60 minutes a day for children and 150 minutes spread through the week for adults).
The food industry can play a significant role in promoting healthy diets by:
- reducing the fat, sugar and salt content of processed foods
- ensuring that healthy and nutritious choices are available and affordable to all consumers
- restricting marketing of foods high in sugars, salt and fats, especially those foods aimed at children and teenager
- ensuring the availability of healthy food choices and supporting regular physical activity practice in the workplace.
Functions of Adipose tissue
Whilst obesity is unhealthy, the body needs fat in its various forms for a variety of functions. Cholesterol is the precursor of adrenocortical steroids without which life is impossible. Fatty acids have significant roles to play in brain development, and the list goes on.
White adipose tissue (WAT)16 stores energy and is also considered to be an endocrine gland that produces leptin and bioactive adipokines (adiponectin, resistin, apelin, visfatin) which take part in glucose and lipid metabolism and cytokines TNF and IL 6 which are pro-inflammatory (can cause insulin resistance) .
- Energy Storage – Storing energy as fat is a characteristic of many organisms and can be considered a strategy that humans use in general, but one in which they also demonstrate substantial variability5
- Production of adipokines
- Adiponectin is a polypeptide hormone of antidiabetic, anti-inflammatory and anti-atherogenic activity. It plays a key role in carbohydrate and fat metabolism.
- Resistin exerts a counter effect compared to adiponectin and its physiological role is to maintain fasting glycaemia.
- Visfatin stimulates insulin secretion and increases insulin sensitivity and glucose uptake by muscle cells and adipocytes
- Apelin probably increases the insulin sensitivity of tissues
- TNF evokes insulin resistance by blocking insulin receptors and inhibits insulin secretion.
- Il-6 causes insulin resistance by decreasing the expression of insulin receptors, decreases adipogenesis and adiponectin and visfatin secretion, and stimulates hepatic gluconeogenesis.
- The fasting-induced hormone asprosin17 is released by adipose tissue and stimulates hepatic glycogenolysis; it can cross the blood-brain barrier and affect the appetite centre of the brain. into the blood stream. Raised levels of asprosin are associated with insulin resistance. When antibodies targeting asprosin are injected into diabetic mice, blood glucose and insulin levels improve, thereby treating the underlying diabetes. Clinical trials are now under way to treat T2DM with anti-asprosin antibodies.
- Production of growth factors – Angiopoietin-1, Fibroblast growth factors, Epidermal growth factor-like growth factor, Hepatocyte growth factor. Insulin-like growth factor, Nerve growth factor, Platelet-derived growth factor

References
- SERMO ( 2015) The History of Obesity – The Renaissance to 1910 ( July 2, 2015)
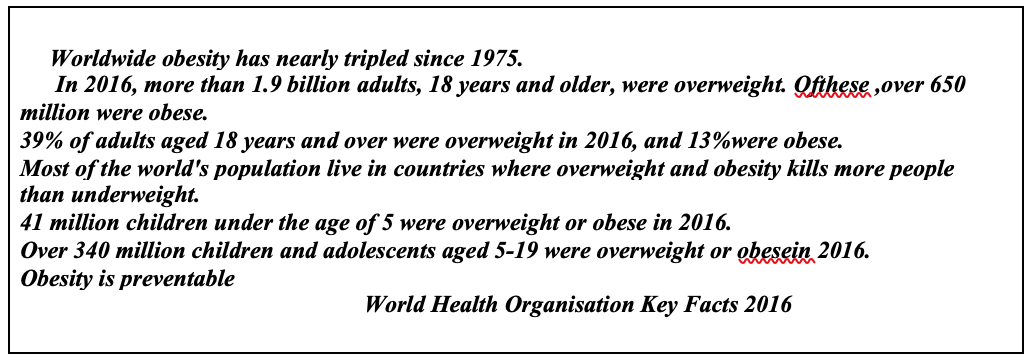
- Obesity and overweight – World Health Organization https://www.who.int › News › Fact
sheets . 16 February 2018 - Danaei G., Ding E. L., Mozaffarian D., Taylor B., Rehm J., Murray C. J., Ezzati M. (2009). The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS. Med.6, e1000058.
- Genetics plays a role in obesity www.obesity.ulaval.ca/obesity/generalities/genetic.php
- Wells JC (2012) The evolution of human adiposity and obesity: where did it all go wrong? Dis Model Mech. 2012 Sep; 5(5): 595–607
- Dokken BB & Tsu-Shuen Tsao ( 2007). The Physiology of Body Weight Regulation: Are We Too Efficient for Our Own Good? Diabetes Spectrum 2007 Jul; 20(3): 166-170. https://doi.org/10.2337/diaspect.20.3.166
- Marks DF ( 2015).Homeostatic theory of obesity.Health Psychol Open. 2015 Jan; 2(1): 2055102915590692.
- Ghanemi A., Yoshioka M., & St-Amand J ( 2018). Broken Energy Homeostasis and Obesity Pathogenesis: The Surrounding Concepts https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6262529/ Nov 2018
- Ogilvie R.P., Patel S.R. The epidemiology of sleep and obesity. Sleep Health. 2017;3:383–388. doi:
- 1016/j.sleh.2017.07.013. [PMC free article] [PubMed10. Jais A & Bruning J ( 2017).Hypothalamic inflammation in obesity and metabolic disease . J Clin Invest.127(1):24-32.
- Acosta A., Port J D ., Abu Dayyeh BK., Camilleri M ( 2014). Recent advances in clinical practice challenges and opportunities in the management of obesity Literature Review . Gut 63(4)
- Common Types of Eating Disorders (and Their Symptoms) – Healthline https://www.healthline.com/nutrition/common-eating-disorders Sep 2018
- Weaver JU ( 2008).. Classical endocrine diseases causing obesity. – NCBI https://www.ncbi.nlm.nih.gov/pubmed/18230905
- Lake A., & Townsend T (2006). Obesogenic environments: exploring the built and food environments. J R Soc Promot Health. 2006 Nov;126(6):262-7
- Hopkins M., Blundell J., Halford J., King N., and Finlayson G ( 2016). The Regulation of Food Intake in Humans. www.endotext.org
- Kuryszko J, Sławuta P, Sapikowski G ( 2016) Secretory function of adipose tissue Pol J Vet Sci. 2016;19(2):441-6. doi: 10.1515/pjvs-2016-0056
- The multi-tasking nature of the hormone asprosin https://blogs.bcm.edu/2018/01/19/the-multi-tasking-nature-of-the-hormone-asprosin/ Jan 2018
Hla Yee Yee1 and Htet Htet Oo2