Introduction
Constipation is a common and debilitating problem worldwide. It affects twice as many women as men.1 Constipation can be defined as a delay or difficulty in defecation. It occurs in all age groups and can be problematic in elderly, pregnancy, and immobility. The prevalence of constipation is estimated to be 11% – 38% of pregnancies and it is relieved in puerperium.2 It affects 21% of all non-pregnant women and higher in menopausal women. Severe constipation may result in faecal impaction, retention of urine, pain or abdominal discomfort, haemorrhoids, anal fissure, rectal bleeding and /or rectal prolapse. Treatment of chronic constipation can be difficult and some cases require long term treatment. In 2010, over 15.9 million prescriptions were dispensed in the community in England for laxatives at the cost of £ 70.6 million.3
Classification
The standard clinical measures commonly used for classification of constipation is Rome IV criteria (Table 1) 4, although it is not specifically designed for pregnancy, a more simplified criteria is used. Constipation is classified as primary (Functional) constipation which is defined as infrequent bowel motion and/or difficulty in passing stool which is not attributable to an underlying pathology. Secondary constipation results from either pharmacotherapy or a medical condition. Medical conditions include primary disease of gastrointestinal tract (such as anal fissure, colorectal strictures and neoplasia), metabolic disturbances (such as hypothyroidism, hypercalcaemia) and neurological disorders. Some may suffer from irritable bowel syndrome associated with constipation (IBS-C).5
Table 1. Rome IV criteria for constipation 4
Patient must experience at least two of the following symptoms over the preceding three months
- Fewer than three spontaneous bowel movements per week.
- Straining for more than 25% of defecation attempts.
- Lumpy or hard stools for at least 25% of defecation attempts.
- Sensation of anorectal obstruction or blockage for at least 25% of defecation attempts.
- Sensation of incomplete defecation for at least 25% of defecation attempts.
- Manual maneuvering required to defecate for at least 25% of defecation attempts.
- Patients should not meet the suggested criteria for Irritable bowel syndrome and loose stool are rarely present without the use of laxatives
The American Gastroenterological Association criteria which utilize colonic transit and anorectal tests to classify into three groups, normal transit constipation (NTC), slow transit constipation (STC), pelvic floor dysfunction or defecatory disorders (DD). It is not commonly used in obstetrics as colonic transit time study is not done in pregnancy.6
Prevalence
Constipation affects up to 11-38% of pregnancies and relieved in puerperium.2 Pregnant women are more prone to constipation in the first two trimesters. The prevalence of functional constipation in the first and second trimester varies between 35% and 39% and 21% in third trimester and 17% in puerperium.7 The prevalence of constipation was lower after vaginal delivery delivery (47%) than caesarean section (57%). One month postpartum, the prevalence of constipation was low, 9% after vaginal delivery and 15% after caesarean section.8
Causes of constipation
The changes in the levels of hormones particularly increased progesterone levels in pregnancy are responsible for reduced intestinal smooth muscle motility. The secretion of peptide hormone motilin which stimulates smooth muscle motility is inhibited by the rise in progesterone and somatostatin. Relaxin which relaxes the myometrium also contributes to the intestinal gut hypomotility. The renin angiotensin system is activated in pregnancy due to high levels of oestrogen and progesterone which stimulate renin and aldosterone. Aldosterone stimulates sodium and water reabsorption from the renal tract and the gut and reduced water content leads to hardened stools. The transit of faeces becomes sluggish secondary to the passive movements of the intestinal tract and uterus eventually leading to constipation.5 Other factors responsible for constipation in pregnancy are mechanical pressure of the gravid uterus, dietary changes (less water and fibre such as non-starch polysacchasides), iron supplements, reduced level of exercise, haemorrhoids, anal fissures, excessive straining which damage the pudendal nerve leading to weakening of the pelvic floor musculature and pain at the episiotomy site also contribute to increased risk of constipation in pregnancy and puerperium.8
Constipation is common in menopause as a result of relaxation of smooth muscles and prolonged transit time. Moreover, constipation in gynaecology can be due to the pressure of pelvic tumours like myoma and ovarian tumours. Rectocele can also cause difficulty in defecation and sense of incomplete defecation as faeces collect in the pouch of rectocele. Pelvic floor dysfunction can also cause defecatory disorder.
Diagnosis
Thorough history taking and physical examination are essential for correct diagnosis and treatment. Key symptoms include infrequent evacuation, passing dry hard stools associated with pain and straining. In addition, history of incomplete evacuation, requirement of digital manipulation in severe cases, presence of symptoms prior to pregnancy or first appearance in pregnancy, worsening in pregnancy, history of laxative or enema use together with the dosage and frequency of treatment should also be noted. Presence of comorbidities such as hypothyroidism, hypercalcaemia, diabetes mellitis, neurological disorders should be recorded. Other bowel conditions like haemorrhoids, anal fissures, neoplasias such as cancer colon and rectum and irritable bowel syndrome (IBS) may require the input from a colorectal surgeon or gastroenterologist.10
Treatment
In the majority of cases, patient education, lifestyle and dietary modification, increasing dietary fibre and fluid intake, moderate exercise and reassurance that these symptoms are transient and normal during pregnancy may be all that is required.
Laxatives are recommended if dietary modifications fail to improve the symptoms. A laxative that is effective, non-teratogenic, not excreted in breast milk and well tolerated should be chosen.
Probiotics may also improve bowel function by conditioning the bowel flora. Antispasmodics and anticholinergics used in IBS are contraindicated in pregnancy and should not be used.9
Bulk-forming laxatives
Bulk-forming laxatives relieve constipation by bulking faecal mass thereby stimulating peristalsis. They are not absorbed from the gastrointestinal tract making them one of the safest and most suitable laxatives for use during pregnancy. This group comprises wheat bran, ispaghula husk, methylcellulose and sterculia. No adverse effects on the fetus have been reported.11 Women should be advised that bulk-forming agents act slowly and therefore can take a few days before the benefit is noticeable. These agents may not always be effective in improving acute symptoms and is contraindicated in faecal impaction.
Osmotic laxatives
Osmotic laxatives comprise lactulose, sorbitol, polyethyleneglycol (PEG), magnesium sulphate or citrate or hydroxide (Milk of magnesia), and salts (sodium chloride, potassium chloride). They act by increasing osmolar tension, resulting in an increased amount of water in the colon facilitating peristalsis and evacuation. Lactulose and PEG are poorly absorbed systemically. PEG is approved by the American Gastroenterology Association and is the treatment of choice for chronic constipation in pregnancy. Common side effects are flatulence and abdominal bloating as hyperosmolar laxatives are indigestible sugars that ferment in the gastrointestinal tract producing excess gas. Although no published studies exist on adverse fetal effects, preclinical data suggest that there is no increased risk of teratogenicity.11 Lactulose is a semi-synthetic disaccharide and is best avoided in women with diabetes and those requiring a low galactose diet. Theoretically, prolonged use of osmotic laxatives might lead to electrolyte imbalances.
Macrogols are inert polymers of ethylene glycol, which sequester fluid in the bowel. It is licensed for use in pregnancy despite limited information in pregnancy, as the effects on the fetus of systemic exposure to the drug are believed to be negligible.1
Stimulant laxatives
Stimulant laxatives such as bisacodyl and senna act regionally within the large intestine by reducing water absorption and causing colonic hyper motility. Stimulant laxatives are more effective than bulk-forming laxatives. However, stimulant laxatives should be used with caution in the third trimester as they can stimulate uterine contractions. This has been documented in several anthraquinone derivatives, though not senna itself 11. Senna is partially absorbed from the gastrointestinal tract. A large case-control surveillance study reported no increased risk of congenital abnormalities. Senna can be excreted in breast milk and hence caution is advised if the woman is breastfeeding. There is minimal absorption (5%) of bisacodyl as it has poor bioavailability. Bisacodyl has not been associated with either teratogenic or fetotoxic effects and is considered suitable for use in pregnancy.11 Docusate sodium acts both as a stimulant and as a softening agent. It is an anionic wetting agent allowing penetration of accumulated hard, dry stool by water and salts. A case of neonatal hypomagnesaemia after maternal overuse of docusate sodium has been reported.11 Therefore, the use of docusate sodium should only be considered at low doses in pregnancy if other treatments are unsuccessful.12 It is excreted in breast milk with oral administration of docusate sodium. Hence, it should be used with caution in lactating mothers.
New agents
Prucalopride stimulates the serotonin 5-HT4 receptor thereby altering colonic motility which provides the propulsive force for defaecation. In 2010 the National Institute for Health and Care Excellence (NICE) approved the use of prucalopride for the management of chronic constipation in women if treatment with two different types of laxatives at maximum dose for a minimum period of 6 months had failed and were being considered for invasive treatment. There are limited data available on its use in pregnancy. It is therefore not recommended during pregnancy and breast feeding. Women of child bearing age should use effective contraception during treatment with prucalopride.13 Newer drugs such as linaclotide and lubiprostone are pregnancy category C drugs, which means that their use should only be considered if the inherent benefits outweigh the possible risks to the fetus. Linaclotide is a guanylatecyclase-C receptor agonist. Its use has been approved for the management of moderate to severe irritable bowel syndrome associated with constipation (IBS-C). The mode of action is by augmenting the concentration of extracellular cyclicguanosine monophosphate (c-GMP), which is thought to reduce visceral pain by decreasing pain fibre activity. In addition, it also increases the concentration of intracellular c-GMP resulting in increasing secretion of electrolytes (chloride and bicarbonate) into the intestinal lumen leading to increased intestinal fluid to ease and accelerate passage of stool. It is metabolised within the gastrointestinal tract and is virtually undetectable in plasma after therapeutic doses. There is a dearth of information available for use during pregnancy or breast feeding. Lubiprostone is a locally acting CIC-2 chloride-channel activator, which augments intestinal fluid secretion and increases motility. It is licensed and approved by NICE for the management of chronic idiopathic constipation if treatment with two different types of laxative at maximum dose for a minimum period of 6 months have failed and invasive treatment is being considered. In animal experimentation, maternal toxicity and over-dosage (higher than recommended human maximum dose) have detected adverse fetal effects. It is unascertained whether these drugs are excreted in breast milk and therefore should be used with caution.13
Suppositories and enemas
Patients suffering from faecal loading or impaction may benefit from use of glycerine suppositories in addition to the use of oral laxatives as necessary. The UK Teratology Information Service advises that glycerine suppositories can be used in pregnancy. No published studies exist regardingthe use of phosphate enemas during pregnancy and potential for teratogenicity.11
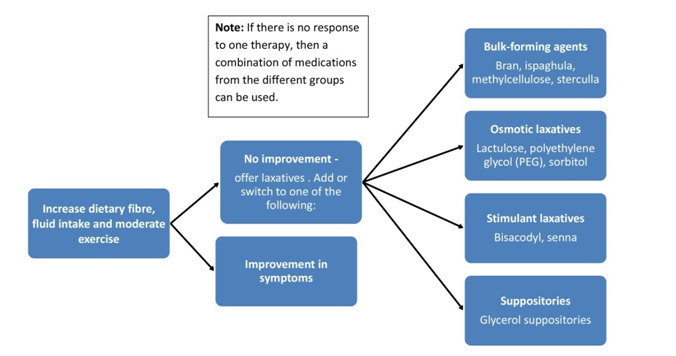
Figure 1. Algorithm for the management of constipation in pregnancy
How to stop laxatives
When regular bowel movements occur without difficulty, laxatives can be withdrawn gradually. The reduction in the dose of laxatives should be guided by the frequency and consistency of the stools. Gradual withdrawal will reduce the risk of requiring re-initiation of therapy for recurrent faecal loading. If a combination of laxatives is used, one laxative should be stopped at a time, reducing stimulant laxatives first. Patients should be aware that the process of weaning off laxatives may take several months. Relapses often occur and are managed by increasing the dose of laxatives promptly. Individuals with a medical or pharmacological cause of constipation may require long-term continued usage of laxatives.5
Non pharmacological managements
Abdominal massage can increase colonic transit time, stimulate peristalsis and lower the pain and discomfort associated with constipation. Digital evacuation relieves faecal impaction.
Surgical treatment
Surgery is indicated for treatment of haemorrhoids, anal fissures, rectal prolapse and neoplasias. Haemorrhoids are usually relieved with conservative measures such as high fibre diet, topical creams, suppositories, pain killers and laxatives. Prolapsed piles and thrombotic piles will need surgery.
Management of constipation in Gynaecology
Pelvic tumours need surgical removal and rectocele should be repaired. Health education, life style and dietary changes, increasing dietary fibres and fluid intake, moderate exercise and reassurance are required for constipation in menopause after excluding gastrointestinal pathologies.
Conclusion
A detailed history and thorough physical examination play a key role in diagnosing and managing women with constipation in pregnancy and non pregnant women effectively. If there are any red flag signs and symptoms women should undergo further investigation to rule out any serious gastrointestinal pathology. A change in bowel habit for longer than 6 weeks, rectal bleeding, known history of gastrointestinal disorders such as inflammatory bowel disease, a family history of colorectal cancer warrant a prompt referral to a gastroenterologist or colorectal surgeon.9
The first-line therapy for constipation should commence by increasing dietary fibre and water intake and moderate exercise. If the first step is unsuccessful in alleviating symptoms then laxatives should be considered (Figure 1). Care must be taken to use the best type of laxative to treat their symptom with minimal risk profile for the mother and baby in pregnancy. Laxatives should be weaned gradually. Women should be advised that it can take several months to be successfully weaned off all laxatives.1
References
- National Institute of Health and Care Excellance, Constipation: Clinical Knowledge Summaries, London, NICE; 2014. http://cks.nice.org.uk/constipation.
- Jewell DJ, Young G. Interventions for treating constipation in pregnancy. Cochrane Database Syst Rev, 2001 (2): CD001142.
- Health and Social Care Information Centre. Prescriptions Dispensed in the Community, Statistics for England, 2000–2010. Leeds: HSCIC; 2011. http://www.hscic.gov.uk/pubs/ presdisp2000-10.
- Simren M, Palsson OS, Whitehead WE. Update on Rome IV criteria for colorectal disorders: Implications for clinical practice. Curr Gastroenterol Rep, 2017; 19 (4): 15.
- Verghese TS, Futaba K, Latthe P. Constipation in Pregnancy. The Obstetrician & Gynaecologist, 2015; 17: 111-115.
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology 2006; 130: 1480-1491.
- Derbyshire E, Davies J, Costarelli V, Dettmar P. Diet, physical inactivity and the prevalence of constipation throughout and after pregnancy. Matern Child Nutr, 2006; 2: 127-134.
- Kuronen M, Hantunen S, Alanne L, Kokki H, Saukko C, Sjovall S, Vesterinen K, Kokki M. Pregnancy, puerperium and perinatal constipation – an observational hybrid survey on pregnant women and their age-matched non-pregnant controls. BJOG, 2021, 128 (6): 1057-1064.
- Turawa EB, Musekiwa A, Rohwer AC. Interventions for treating postpartum constipation. Cochrane Database Syst Rev, 2020; (8): CD011625.
- Longo SA, Moore RC, Canzoneri BJ, Robichaux A. Gastrointestinal conditions during pregnancy. Clin Colon Rectal Surg, 2010; 23: 80-89.
- UK Teratology Information Service. Treatment of Constipation in Pregnancy. Newcastle: UKTIS; 2014. http://www.uktis.org/docs/Constipation.pdf.
- Van Tonningen M. Constipation during pregnancy. In: Schaefer C PP, Miller RK, editors. Drugs During Pregnancy and Lactation: Treatment Options and Risk Assessment. 2nd ed. London: Academic Press; 2007.
- National Institute for Health and Care Excellence. Prucalopride for the Treatment of Chronic Constipation in Women. NICE Technology Appraisal Guidance 211. London: NICE, 2010 https://www.nice.org.uk/guidance/ta2.
Author Information
Yin Yin Soe
Retired Professor, Department of Obstetrics and Gynaecology, University of Medicine (1), Yangon
Chief Editor, Myanmar Medical Journal