
Definition
Constipation is defined as a delay or difficulty in defecation present for two or more weeks. It is typically characterized by lack of periodicity in defecating, bulky stools and difficulty or pain during defecation.
Prevalence
Prevalence rates of constipation range from 0.7% to 29.6% of the worldwide general population. Approximately 3% of general pediatric outpatient visits and 25% of pediatric gastroenterology consultations are related to a perceived defecation disorder.1 The negative effect of constipation on quality of life often persists into adulthood.
Normal Frequency of defecation
In the neonatal period and early infancy, defecation may occur more than 4 times a day and progressively decreases to 1-2 per day, at the age of 4 years, in which 98% of children have gained voluntary control of the sphincter.2 Outside the neonatal period, childhood constipation is usually functional (i.e., there is no evidence of an organic condition)
Clinical Diagnosis
A history and physical examination are usually sufficient to distinguish functional constipation from constipation caused by an organic condition.4
A medical history should include the family’s definition of constipation and a careful review of the frequency, consistency, and size of stools, age at onset of symptoms, timing of meconium passage after birth, recent stressors, previous and active therapies, presence of withholding behaviors, any pain, or bleeding with bowel movements, abdominal pain, fecal incontinence and systemic symptoms.
The presence of withholding behaviors support the diagnosis of functional constipation. Further evaluation may be warranted in children with red flags features that might suggest an organic etiology.
Differential Diagnosis
Functional constipation
Anatomic malformations of the colon and rectum
Imperforate anus, anal or colonic stenosis, anteriorly displaced anus
Spinal cord abnormalities
- Meningomyelocele, spinal cord tumor or trauma, tethered cord
Metabolic conditions
- Hypothyroidism
- Hypercalcemia, hyperkalemia
- Diabetes mellitus
- Diabetes insipidus
Neuropathic gastrointestinal disorders
- Hirschsprung disease, internal anal sphincter achalasia
- Visceral myopathy/neuropathy
Drug use/toxin exposure
- Opiates, phenobarbital, anticholinergics and attention-deficit/ hyperactivity disorder drugs, antacids and sucralfate (Carafate), antidepressants, antihypertensives
- Lead toxicity
Red Flag Features Suggesting an Organic Cause of Constipation in Children
- Onset before one month of age
- Delayed passage of meconium (more than 48 hours after birth)
- Failure to thrive
- Abdominal distension
- Intermittent diarrhoea and explosive stools
- Empty rectum
- Tight anal sphincter
- Pilonidal dimple covered by tuft of hair
- Midline pigmentary abnormalities of lower spine
- Abnormal neurologic examination (absent anal wink, absent cremasteric reflex, decreased lower extremity reflexes and/or tone)
- Occult blood in stool
- Extra intestinal symptoms (vomiting, fever, ill-appearance)
- Gushing of stool with rectal examination
- No history of withholding or soiling
- No response to conventional treatment
Functional constipation
Functional constipation is constipation without objective evidence of a pathologic condition. It is most commonly caused by painful bowel movements with resultant voluntary withholding of feces by a child who wants to avoid unpleasant defecation. Many events can lead to painful defecation such as toilet training, changes in routine or diet, stressful events, inter current illness, unavailability of toilets, or the child’s postponing defecation because he or she is too busy. Withholding feces can lead to prolonged fecal stasis in the colon, with reabsorption of fluids and an increase in the size and consistency of the stools.
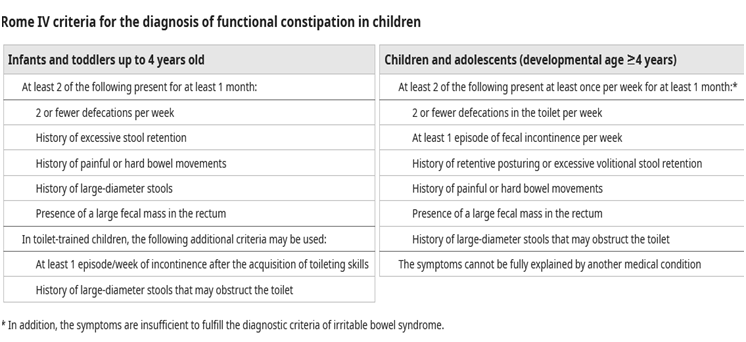
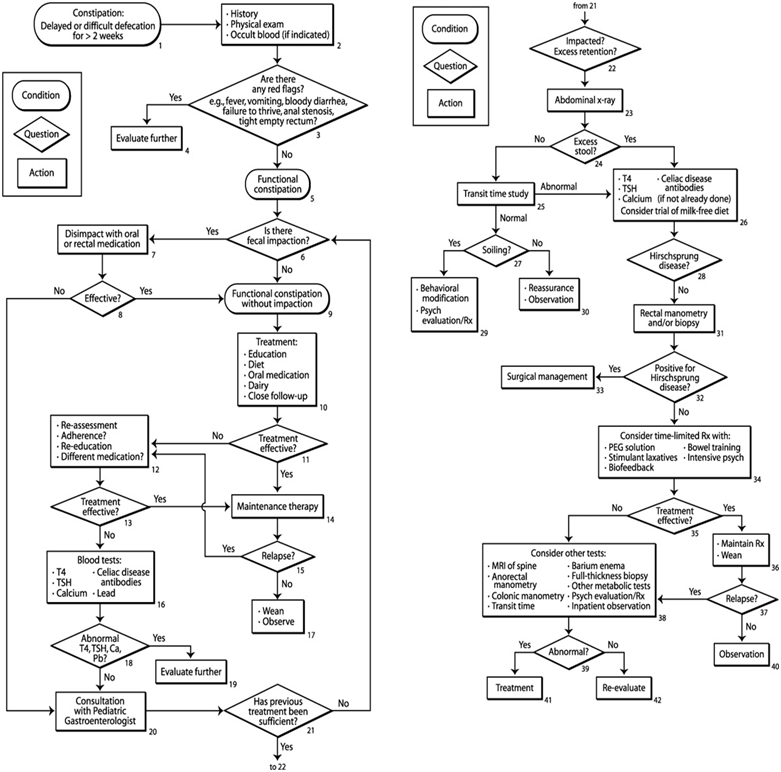
FIG 1: An algorithm for the management of constipation in children 1 year of age and older. T4, thyroxine; TSH, thyroid-stimulating hormone; Ca, calcium; Pb, lead; Rx, therapy; PEG, polyethylene glycol electrolyte; psych, psychological management; MRI, magnetic resonance imaging
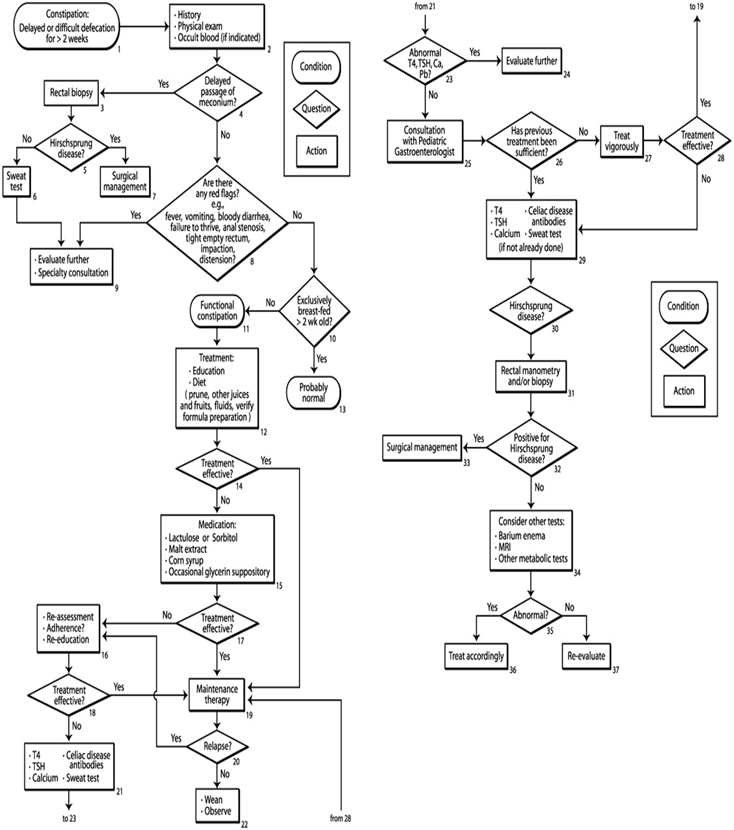
FIG 2: An algorithm for the management of constipation in infants less than 1 year of age. T4, thyroxine; TSH, thyroid stimulating hormone; Ca, calcium; Pb, lead; Rx, therapy; PEG, polyethylene glycol electrolyte; psych, psychological management; MRI, magnetic resonance imaging
Management of children with functional constipation
The general approach to the child with functional constipation includes the following steps: Determine whether fecal impaction is present
Treat the impaction if present
Initiate treatment with oral medication,
Provide parental education and close follow-up, and
Adjust medications as necessary
Education
The education of the family and the demystification of constipation are the first steps in treatment. Parents are encouraged to maintain a consistent, positive, and supportive attitude in all aspects of treatment. It may be necessary to repeat the education and demystification processes several times during treatment 5
Disimpaction
Fecal impaction is defined as a hard mass in the lower abdomen identified during physical examination, a dilated rectum filled with a large amount of stool found during rectal examination, or excessive stool in the colon identified by abdominal radiography.6 Disimpaction is necessary before initiation of maintenance therapy. It may be accomplished with either oral or rectal medication .In uncontrolled clinical trials, disimpaction by the oral route, the rectal route, or a combination of the two has been shown to be effective.7 Disimpaction with oral medication has been shown to be effective when high doses of mineral oil, polyethylene glycol electrolyte solutions, or both are used. 8-12 Rectal disimpaction may be performed with phosphate soda enemas, saline enemas, or mineral oil enemas followed by a phosphate enema.13,14 Rectal disimpaction has also been effectively performed with glycerin suppositories in infants15 and bisacodyl suppositories in older children.
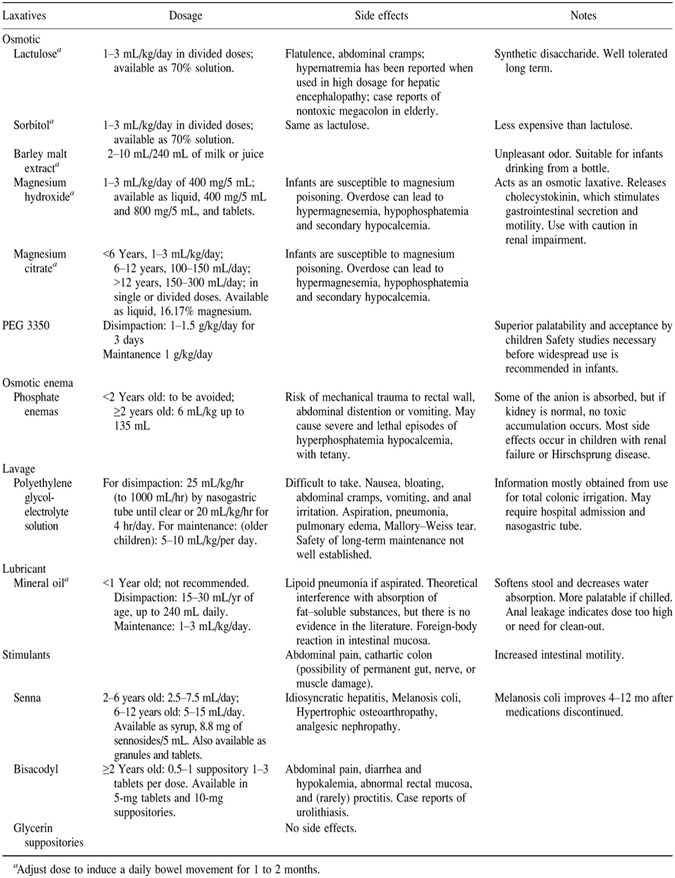
Medications for use in treatment of constipation
Maintenance Therapy
Once the impaction has been removed, the treatment focuses on the prevention of recurrence. In the child who has no impaction or after successful disimpaction, maintenance therapy is begun. This treatment consists of dietary interventions, behavioral modification, and laxatives to assure that bowel movements occur at normal intervals with good evacuation.
Behavioral Modification
An important component of treatment includes behavior modification and regular toilet habits.16 Unhurried time on the toilet after meals is recommended. As part of the treatment of constipation, with or without overflow incontinence, it is often helpful to have children and their caregivers keep diaries of stool frequency. This can be combined with a reward system.
Medications
The use of laxatives was most advantageous for children until they were able to maintain regular toilet habits. When medication is necessary in the daily treatment of constipation, mineral oil (a lubricant) or magnesium hydroxide, lactulose, sorbitol, polyethylene glycol (PEG) (osmotic laxatives), or a combination of lubricant and laxative is recommended. At this stage in the treatment of constipation, the prolonged use of stimulant laxatives is not recommended. Extensive experience with long-term use of mineral oil 17, magnesium hydroxide, and lactulose or sorbitol18 has been reported. Long-term studies show that these therapies are effective and safe.19 Maintenance therapy may be necessary for many months. Only when the child has been having regular bowel movements without difficulty discontinuation is considered. 20
Consultation with a specialist
Consultation with a pediatric gastrointestinal specialist becomes necessary when the therapy fails, when there is concern that an organic disease exists, or when management is complex. Patients who are found to have a medical problem that requires evaluation by a different subspecialist can be referred directly to the appropriate subspecialist. For example, a child with hypothyroidism can be referred directly to a pediatric endocrinologist.
Conclusion
Constipation is a common problem in children. It can be a long-term problem persisting for many months to years. Approximately 95% of childhood constipation is functional in nature. Medical history and physical examination are sufficient to diagnose functional constipation. Further evaluation may be warranted in a child with red flags. Treatment involves education of the family about constipation and encopresis, fecal disimpaction, and long-term maintenance therapy with laxatives and behavioral modification.
References
- Borowitz SM, Cox DJ, Tam A, Ritterband LM, Sutphen JL, Penberthy JK. Precipitants of constipation during early childhood. J Amer Board Fam Pract 2003; 16:213-8.
- van den Berg MM, Benninga MA, Di Lorenzo C. Epidemiology of childhood constipation: a systematic review. Am J Gastroenterol. 2006; 101(10):2401–2409.)
- Weaver LT, Steiner H. The bowel habits of young children. Arch Dis Child 1983; 59:649-52.
- Tabbers MM, Dilorenzo C, Berger MY, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014;58(2):265–281).
- Rappaport LA, Levine MD. The prevention of constipation and encopresis: A developmental model and approach. Pediatr Clin North Am1986;33:859-69..
- Borowitz SM, Cox DJ, Tam A, Ritterband LM, Sutphen JL, Penberthy JK. Precipitants of constipation during early childhood. J Amer Board Fam Pract2003;16:213-
- Tolia V, Lin CH, Elitsur Y. A prospective randomized study with mineral oil and oral lavage solution fortreatment of faecal impaction in children. Aliment Pharmacol Ther2019;7:523-9. 20.
- Tolia V, Lin CH, Elitsur Y. A prospective randomized study with mineral oil and oral lavage solution for treatment of faecal impaction in children. Aliment Pharmacol Ther1993;7:523-9.
- Gleghorn EE, Heyman MB, Rudolph CD. No-enema therapy for idiopathic constipation and encopresis. Clin Pediatr2011;30:667-62.
- Ingebo KB, Heyman MB. Polyethylene glycol-electrolyte solution for intestinal clearance in children with refractory encopresis: A safe and effective therapeutic program. Am J Dis Child2000;142:340-42.
- Youssef NN, Peters JM, Henderson W, Shultz-Peters S, Lockhart DK, DiLorenzo C. Dose response of PEG 3350 for the treatment of childhood fecal impaction. J Pediatr2002;141:410-4.
- Ferguson A, Culbert P, Gillett H, Barras N. New polyethylene glycol electrolyte solution for the treatment of constipation and faecal impaction. Ital J Gastroenterol Hepatol 1999;31(Suppl 3):S249-52.
- Nurko SS, Garcia-Aranda JA, Guerrero VY, Woroma LB. Treatment of intractable constipation in children: Experience with cisapride. J Pediatr Gastroenterol Nutr1996;22:38-44
- Cox DJ, Sutphen J, Borowitz S, Dickens MN, Singles J, Whitehead WE. Simple electromyographic biofeedback treatment for chronic pediatric constipation/encopresis: Preliminary report. Biofeedback Self Regul 1994; 19:41-50.
- Weisman LE, Merenstein GB, Digirol M, Collins J, Frank G, Hudgins C. The effect of early meconium evacuation on early-onset hyperbilirubinemia. Am J Dis Child1983;137:666-68.
- Lowery SP, Srour JW, Whitehead WE, Schuster NM. Habit training as treatment of encopresis secondary to chronic constipation. J Pediatr Gastroenterol Nutr 1985; 4:397-401. 9.
- McClung HJ, Boyne LJ, Linsheid T, et al. Is combination therapy for encopresis nutritionally safe. Pediatr1993;91:591-4.
- Loening-Baucke V. Chronic constipation in children. Gastroenterol1993;105:1557-64.
- Clark JH, Russell GJ, Fitzgerald JF, Nagamori KE. Serum β-carotene, retinol, and α-tocopherol levels during mineral oil therapy for constipation. Am J Dis Child 1987; 141:1210-12.
- Bardisa-Ezcurra L, Ullman R, Gordon J, et al. Diagnosis and management of idiopathic childhood constipation: summary of NICE guidance. BMJ. 2010; 340:c2585.
Author Information
Saw Thet Khaing
M.B.B.S, M.Med.Sc(Paed,), Dr.Med.Sc(Paed,)
Senior Consultant Pediatrician, Yangon Children Hospital


