

Introduction
The amyloidoses are a group of rare diseases that have in common the extracellular deposition of pathologic, insoluble fibrils in various tissues and organs.11 Primary amyloidosis is a monoclonal plasma cell disorder with an incidence of approximately 8 per million per year, its subtypes are classified according to the composition of the amyloid subunit protein.1,3-5 This disease has a male preponderance of 60% to 65% and affects 99% patients older than 40 years of age.3 Secondary systemic amyloidosis is a disorder in which insoluble protein fibers become deposited in tissues and organs impairing their function. It is found in association with chronic infection or chronic inflammatory disease.4,5,6,7
Chronic diarrhoea is defined as a condition lasting more than four weeks.12 It is one of the most common clinical presentations and underlying cause should be analyzed. Several conditions could determine chronic diarrhoea: bowel resection, drugs (laxatives in particular), infections, endocrinopathies, glucose mal-absorption, chronic mesenteric ischemia, lymphatic obstruction, celiac disease, pancreatic failure, colonic mucosa wall alterations (amyloidosis, Whipple disease, microscopic colitis or collagenous colitis).11
Systemic amyloidosis, however, is often overlooked in the differential diagnosis of malabsorption.1 The most important measure to distinguish primary to secondary amyloidosis is urine or serum protein immunofixation electrophoresis. Bone marrow aspiration and biopsy or fat aspiration could be performed.1-5 When negative, findings for underlying illness related to amyloidosis should be investigated. Colonoscopy commonly reveals mucosal friability and erosions.3,4,8 Hystologic evidence stained with Congo-red (sensitivity of 90%) will demonstrate an apple-green birefringence under polarizing light.1,3-9 This confirms the diagnosis but not the subtype.2
Prognosis depends on the specific type of amyloidosis and the organs involved.2,3-5 The cause of death in most patients is cardiac and kidney related disease.3,4 Hayman et al reported weight loss and low hemoglobin concentration as worse prognostic indicator on gastrointestinal amyloidosis.1 Management should remain supportive, diarrhea may be managed with agents as loperamide and ocreotide.1,9
Case
A 46-year-old married lady presented with chronic diarrhoea of 4 years and admitted to Medical Unit (5) of Yangon General Hospital for evaluation. We noticed that she couldn’t walk because of weakness of both lower limbs for two years. Loose motion started about 4 years ago which was 7-8 times per day of liquid yellow stool and contained mucous and ingested food, not associated with abdominal pain, bloody stool , greasy oily stool, bad odor and fever, approximately 150 ml – 300 ml per motion. No histroy of passing worms or sense of incomplete defecation, No obvious aggrevating factors (like milk, stress, coffee ) or releieving factors. Associated features of postural hypotension such as lightheadedness and fainting when from sitting to standing were present but no features of electrolyte imbalances like muscle cramps, weakness. She had loss of appetite and had total weight loss of 15 kg within 4 years. On acquiring about weakness of limbs, she noticed weakness of both lower limbs, initially affecting the distal muscles which progressed to involve proximal muscles as she was unable to climb stairs and had difficulty getting up from squatting position, and now she was unable to walk or stand on her both feet. She also noticed reduced sensation in both lower limbs and numbness continued to progress resulting in repeated scald of lower limbs and rat bite in all toes. she denied any motor and sensory losses in both upper limbs. No relevant past medical history like diabetes mellitus, hypertension, cerebrovascular accidents, tuberculosis or contact with tuberculosis. No history of surgery. She underwent OGDS in 2021 which revealed normal gastroscopy. She had no regularly taking drugs. She had no history of allergy.
On examination, her BMI was 17.4 kg/m2 with mild pallor, dry tongue, and glossitis. The blood pressure was 120/70 mmHg on lying and 100/60 mmHg on standing. Her heart rate was only 48/min. There was mild oedema on both lower limbs. Scars from scalds and rat bites were detected on both lower limbs. Signs of peripheral neuropathy were present with glove and stocking pattern sensory loss with motor power of 2/5 distally. Other systemic examination findings were unremarkable.
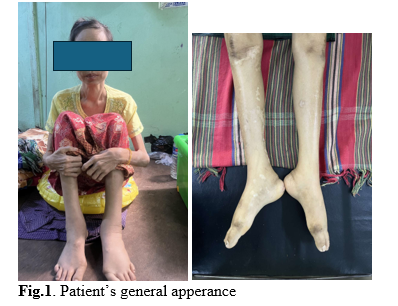
Fig.1. Patient’s general apperance
In summary, a 46-year-old woman presenting with chronic diarrhoea and peripheral neuropathy with orthostatic hypotension and bradycardia.
For infection screening, serology for HIV, anti HBs antibody and anti HCV antibody were negative. Widal test was also negative from 1/20 dilution. Stool for AFB was not seen. Stool RE only showed bacterial flora. Thyroid function tests came back as euthyroid.
Chest Xray showed no obvious abnormality.
USG abdomen only revealed cystitis. Tumor markers CEA was 6.68 ng/ml and CA19-9 elevated at 63.8 U/ml. So, CT abdomen and pelvis was proceeded and revealed cystitis only and lumbar spondylosis and no irregular bowel wall thickening.
We consulted with Department of Gastroenterology of Yangon General Hospital and colonoscopy was planned with rectal biopsy. Normal colonoscopy was seen. Rectal biopsy showed mild proctitis and no features of tuberculosis or inflammatory bowel disease. Congo-red stain detected amyloidosis under ordinary light microscopy and polarized light microscopy.

Fig 3. H&E stain of rectal biopsy

Fig 4. Congo-red stain of rectal biopsy
Nerve conduction study also showed bilateral Carpal-Tunnel Syndrome and symmetrical axonal sensorimotor polyneuropathy which was conducted by Department of Neurology of Yangon General Hospital.
Department of Cardiology of Yangon General Hospital also performed Echocardiogram and commented normal echocardiogram. ECG showed heart block.
To differentiate primary and secondary amyloidosis, after consulting with Department of Haematology, Yangon General Hospital, we proceeded to undergo bone marrow examination which came out as hypoplastic myelodysplastic marrow, and serum protein fixation electrophoresis failed to show oligoclonal bands. For chronic inflammatory conditions, we performed ANA which was 1/100, RA was 5.0 IU/ml (Reference < 14) and anti CCP was <7.00 U/ml (Reference <17). Our final diagnosis was chronic diarrhoea and symmetrical axonal sensorimotor peripheral neuropathy due to amyloidosis. Symptomatic treatments for loose motion and neuropathy were given. But unfortunately, the patient passed away due to arrhythmia due to autonomic neuropathy.
Discussion
This 46-years-old lady, came with chronic diarrhea, whose stool analysis revealed only bacteria flora. Colonoscopy showed normal with histologic result of amyloidosis. Mechanism of chronic diarrhoea in patients with intestinal amyloidosis according to the literature, include autonomic neuropathy, myopathy and dysmotility that lead to bacterial and or fungal overgrowth, vascular invasion, mucosal injury and ischemia.9 Hayman et al stated that malabsorption occurs in less than 5% of patients with systemic amyloidosis with symptoms of diarrhea, steatorrhea, anorexia, dizziness, orthostatis, nausea or abdominal pain.1 Although the rectal biopsy revealed amyloidosis, the protein electrophoresis could not show any abnormal monoclonal immunoglobulin light chains, so amyloidosis in this patient is likely to be secondary cause and primary amyloidosis can be excluded. According to literature, anemia with hemoglobin of 9.9 g/dl and loss of body weight are bad prognostic factors for gastrointestinal amyloidosis.1 In both primary and secondary amyloidosis, the gastrointestinal system is the most involved, with the colon being the most frequently involved organ.8 This case fits in with the literature, where the colonoscopy was found colitis. Other part of the gastrointestinal system which also can be affected is the esophagus, where the muscular and Auerbach plexus can be infiltrated with amyloid. The lower esophageal sphincter’s tone will decrease, peristalsis impaired and cause gastroesophageal reflux.1,8,10 Organ dysfunction results not only from disruption of tissue architecture by amyloid deposits but also from a direct cytotoxic effect given by amyloidogenic precursor proteins or precursor aggregates.15
In this case, we couldn’t find the secondary causes of amyloidosis. In secondary amyloidosis the treatment is towards management of underlying condition to prevent progression of amyloidosis. Aim of treatment is to control the underlying disease and the symptoms.13
Amyloidosis also includes ATTR (Transthyretin amyloidosis) as well as amyloidosis related to plasma cell disorders (AL or light-chain amyloidosis), products of chronic infammation (AA amyloidosis as seen with some chronic infammatory disorders), and organ-specifc amyloidosis such as Alzheimer’s disease.14
Conclusion
The clinical manifestations of amyloidosis that caused by amyloid deposition could be various, which can make misleading diagnosis for many years even after the onset of symptom. Primary or secondary amyloidosis should always be considered in malabsorptive chronic diarrhea. A multidisciplinary approach is essential both to manage symptoms and to help rule out other conditions. Recent guidelines outline the importance of this approach, with early referral to cardiology and neurology being strongly recommended along with involvement from hematology, when appropriate, to rule out plasma cell disorders.
References
- Hayman SR, Lacy MQ, Kyle RA, et al. Primary Systemic Amyloidosis: A cause of malabsorption syndrome. Am J Med. 2001;111: 535-40
- Khan MF, Falk RH. Amyloidosis. Postgrad Med J 2001;77:686-93.
- Gertz MA, Lacy MQ, Dispenzieri A. Amyloidosis. Hem Oncol Clin North Am 1999;13:1211-33.
-
- Jacobson DR. Amyloidosis, overview. Available at:
- Amyloidosis. Available at: http://www.dreddyclinic.com/findinformation/aa/amyloidosis.htm.
- Mor AM, Gal R, Livneh A. Abdominal and digestive system associations of familial mediterranean fever. Am J Gastroenterol 2003;98(12):2594-604.
- Okuda Y, Takasugi K, Oyama T et al. Intractable diarrhea associated with secondary amyloidosis in rheumatoid arthritis. Ann Rheuma Dis 1997;56:535-41.
- Georgiades CS, Neyman EG, Barish MA, et al. Amyloidosis: Review and CT Manifestation. RadioGraphics 2004;24: 405-416.
- Poullos PD, Stollman N. Gastrointestinal Amyloidosis: Approach to Treatment. Curr Treat Opt Gastroenterol 2003;6:17-25
- Levy DJ. Gastrointestinal bleeding and amyloidosis. Am J Gastroenterol 1982;77:422-6.
- C. Fonnesu, m. Giovinale, e. Verrecchia, g. De socio, C. Cerquaglia, v. Curigliano, a. Soriano, l. Obici, a. Grieco, L. Lauriola, g. Gasbarrini, r. Manna. Gastrointestinal amyloidosis: a case of chronic diarrhoea: European Review for Medical and Pharmacological Sciences. 2009;13(Suppl 1): 45-50.
- HARRISON. Principi di medicina interna. XV Edizione 2002.
- Lydia D Simatupang, Kharia Utia, Ari Fahrial Syam, Marcellus Simadibrata, Arya Govinda, Ening Krisnuhoni. Case report: Chronic diarrhoea due to intestinal amyloidosis. The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy. 2005 Volume 6, Number 3.
- Benson MD, Buxbaum JN, Eisenberg DS, et al. Amyloid nomenclature 2018: recommendations by the International Society of Amyloidosis (ISA) nomenclature committee. Amyloid. 2018;25(4):215–9. https://doi.org/10.1080/13506129.2018.1549825.
- SKINNER M, APSTEIN CS, LIAO R. Human amyloidogenic light chains directly impair cardiomyocyte function through an increase in cellular oxidant stress. Circ Res 2004; 94:1008-1010.
Author Information
Kay Kay Khine 1, Phoo Ngon Nay Win 2, San San Win 3, Moe Wint Aung 4
- Postgraduate trainee, Department of Medicine, University of Medicine (1), Yangon.
- Doctoral candidate, Department of Diabetes and Endocrinology, University of Medicine (1), Yangon.
- Professor, Department of Diabetes and Endocrinology, Yangon General Hospital.
- Professor and Head, Department of Diabetes and Endocrinology, University of Medicine (1), Yangon.

