Introduction
The burden of stroke in Myanmar has increased during the past decades and stroke was the most common reason for admission to Neurology department of Yangon General Hospital in recent years.1 Stroke remains the second leading cause of death and the third leading cause of combined death and disability in the world. Among the two main types of stroke, ischemic stroke constitutes about three quarters of cases.
Reperfusion therapies
The main goal of reperfusion therapy is to restore blood perfusion to the regions of brain that are ischemic (ischemic penumbra) but not yet infarcted. There are two options for reperfusion therapy that are proven effective in acute ischemic stroke, intravenous thrombolysis (IVT) and mechanical thrombectomy (MT). Intravenous thrombolysis (IVT) using recombinant tissue plasminogen activator (tPA) improves functional outcome when given within 4.5 hours of ischemic stroke onset. Mechanical thrombectomy is indicated for patients with acute ischemic stroke due to large artery occlusion (LVO) in the anterior circulation and can be treated within 24 hours of the time last known to be well, regardless of whether they receive IVT or not.
Time is brain/every minute counts
Two million neurons die every minute in acute ischemic stroke if no effective therapy is given in time. The most important factor in successful reperfusion therapy of acute ischemic stroke is early treatment. So it is of utmost importance to timely save or lessen the area of brain damage and subsequently to reduce the disability as well as to improve the quality of life of stroke patients.
Hyper-acute stroke management protocol
Hyper-acute stroke management starts with prehospital recognition and management. Emergency medical responders identify the patients with a suspected stroke, by using a validated stroke screening tool, and transport them rapidly to the nearest hospital that can provide urgent stroke care with the capability to treat with IVT, or IVT and MT. It is important to establish rapid emergency medical services (EMS) system transport and pre-arrival notification to the receiving hospital.
When the patient arrives emergency department (ED) within 4.5 hours from stroke onset, ED doctor assesses the patient with stroke triage protocol (Rosier scale), do the initial assessment and stabilization of airway, breathing and circulation. All adult patients with a clinical diagnosis of acute ischemic stroke should be rapidly screened for treatment with intravenous thrombolysis (IVT). At the same time, nurses do the investigations such as ECG, random blood sugar (RBS), blood for full blood count, INR, APTT, creatinine, urea and electrolytes, grouping and matching (G&M). When the patient met all stroke triage criteria, ED team notify the oncall stroke team as soon as possible, and immediate notification may also be considered for the radiology and pathology departments. As soon as blood taking and initial assessment are finished, patient is sent for urgent CT headscan. When stroke team arrives, the primary role of stroke team consultant is to confirm the stroke and symptom onset, exclude stroke mimics (psychogenic, seizures, hypoglycemia, migraine with aura (complicated migraine), hypertensive encephalopathy, wenicke’s encephalopathy, CNS abscess, CNS tumor, drug toxicity etc.), assess National Institute of Health Stroke Scale (NIHSS) Score (Table 1) and to decide if the patient is eligible for acute therapy (IVT) (Table 2). NIHSS is used to know the distribution and localize the stroke site, to assess the severity (> 15: major stroke, 6-15: moderate stroke, < 6: minor stroke, 0 = normal score) as well as to decide for tPA treatment. After reviewing the CT scan by neurologist and radiologist, and neurologist decided to proceed with intravenous thrombolysis, informed consent must be taken from patient/family after explaining the purpose of therapy and its potential side effects. The dose of intravenous thrombolysis (tPA) is 0.9 mg/kg (maximum total dose of 90 mg) (10% given as an initial bolus over one minute and the remaining 90% to be given as an infusion via syringe pump over 60 minutes immediately after bolus dose ).
All stroke patients received IVT have to be kept and monitored (figure 1) in stroke ICU or HDU for at least 24 hours for close monitoring and management of post-tPA complications.2 The most life-threatening complication is bleeding (intracranial or extracranial) which can be significant and fatal in 6%.3 Second complication is anaphylaxis which is of small percentage.
To lessen bleeding complications, it is necessary to avoid unnecessary interventions like intramuscular injections, bladder catheterization and nasogastric tube insertion until 8 hours post therapy, and to avoid puncture of arteries or large veins within 24 hours, and not to give antiplatelet therapy or anticoagulants within 24 hours. During monitoring, when the GCS drops 2 points or NIHSS rises at least 4 points from baseline score or new headache or vomiting occur in the patient, urgent CT head scan must be done to check for bleeding. Once there is bleeding complication, must consult hematologist immediately and give cryoprecipitate with target fibrinogen level over 1.5g/L and platelets if platelet count < 100 x 109.2 To reduce such complications, it is essential to follow the inclusion and exclusion criteria and to control the blood pressure vigorously with the target of < 185/110 before thrombolysis and < 180/105 during and post thrombolysis.
For patients with ischemic strokes who could not arrive in 4.5 hours from onset but for those within 48 hours of onset, loading dose of antiplatelet should be given.2
Other subsequent management include antiplatelet therapy according to protocol after 24 hours of thrombolysis, lipid lowering agents, BP and blood glucose control and other risk factors management, swallowing assessment and nutrition, bladder and bowel care, posture care, deep vein thrombosis prophylaxis and health education. Last but not least is early rehabilitation. Stroke rehabilitation is the essential part of treatment plan to reduce long term morbidity.
Recommended timelines
Recommended timelines for hyper-acute stroke management are: door to physician < 10 minutes, door to stroke team < 15 minutes, door to CT < 25 minutes, door to CT interpretation < 45 minutes, door to needle (IVT)< 60 minutes and door to stroke unit admission <3 hours.4
Stroke Unit
Evidence form randomized controlled trials and meta-analyses have shown clearly that care in stroke unit significantly reduces death and disability when compared with general medical wards.5 Therefore, treatment of all acute stroke patients in specialized stroke unit is highly recommended. Stroke unit is, not dependent on complex technology, but just an organized in-hospital facility that is devoted for stroke care. It has multidisciplinary team involving persons trained in acute stroke management. A multidisciplinary stroke unit team consists of doctors, nurses, neurologist/ general physician, neurosurgeon, radiologist, pathologist, physiatrist, physiotherapist, speech therapist, dietitian, etc. The benefit of stroke unit is provision of high-quality basic medical care and some specific treatments like IVT. Hyperacute stroke unit (HASU) provides rapid assessment and diagnostic investigations, hyperacute therapeutic interventions, neurological monitoring, secondary prevention and early rehabilitation.
Hospital Characteristics necessary to run Stroke Unit2
- Emergency department operating 24/7 on-site.
- ICU/HDU – Stroke beds, facilities (Ventilator, Cardiac monitor and defibrillator etc.)
- CT scan (≥64 slices) within 30 minutes of hospital admission in all acute stroke patients
- Laboratory test (CBC, PT, APTT, INR, Blood chemistry) – availability 24/7, Report results within 45 minutes of patient arrival
- ECG at any time
- Echocardiogram – available 7 days a week during working hours
- Extracranial and intracranial ultrasonography laboratory available on a 24/7 basis
- IV tPA with target door to needle time < 60 minutes (in hospitals where thrombolysis is available), IV antihypertensive and other essential medicines for emergency
- Access to surgery for hemicraniectomy +/- haematoma evacuation (in hospitals where thrombolysis is available)
- Multidisciplinary stroke team
- In-house rehabilitation service
- Stroke management Protocol forms and documents, Stroke data registry
References
- Ohnmar O, Myat Kyaw; Zarni Myint Shwe; Khin Myat Po Po Kyaw; Moe Zaw Myint; Yan Lynn Aung; Htet Htet Lin; Yin Minn Aye; San Oo; Win Min Thit.2021. “The pattern and burden of neurological disorders: A systemic review of Neurology Department, Yangon General Hospital, Myanmar.” Neurology Asia. 2020, Vol. 25 Issue 4, p555-561. 7p.
- Acute stroke care standard operating procedures, Department of neurology, Yangon General Hospital, Myanmar, 2015.
- Yaghi S, Eisenberger A, Willey JZ. 2014. “Symptomatic intracerebral hemorrhage in acute ischemic stroke after thrombolysis with intravenous recombinant tissue plasminogen activator: a review of natural history and treatment.” JAMA Neurol. 1(9): 1181-5.
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL; 2019. “On behalf of the American Heart Association Stroke Council. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association”. Stroke; 50:e344–e418.
- Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database of Systematic Reviews 2013, Issue 9. Art. No.: CD000197. DOI: 10.1002/14651858.CD000197.pub3. Accessed 26 January 2023.
Table 1. National Institute of Health Stroke Scale (NIHSS) Score Sheet
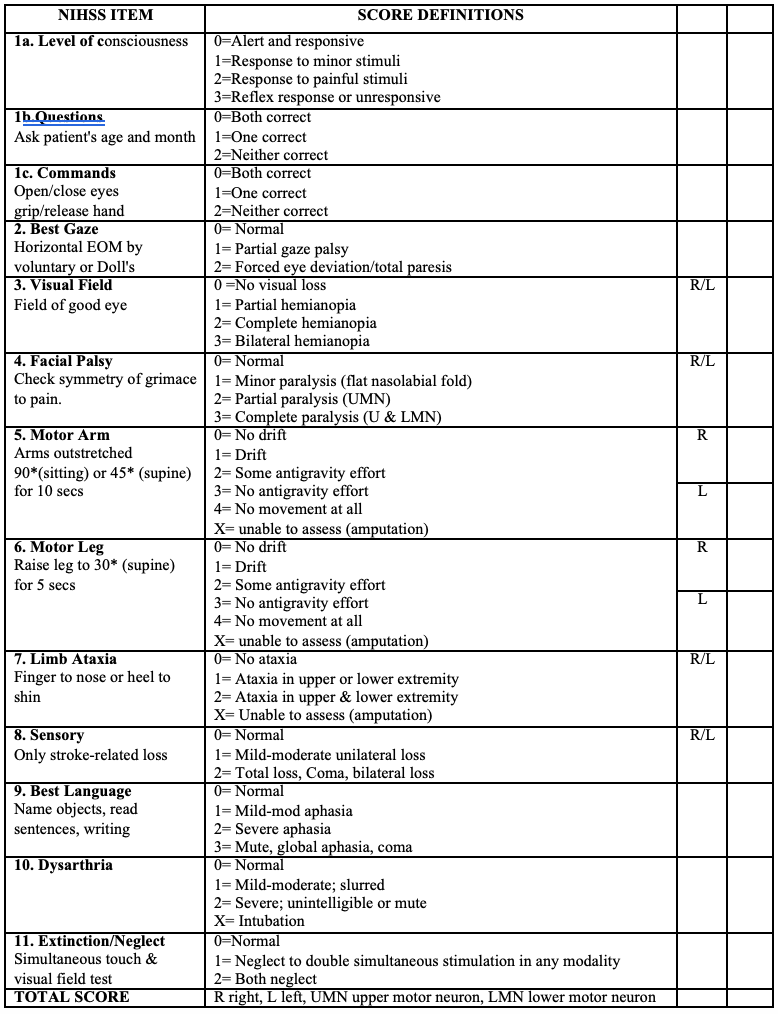
Table 2.Checklist for indications of thrombolysis
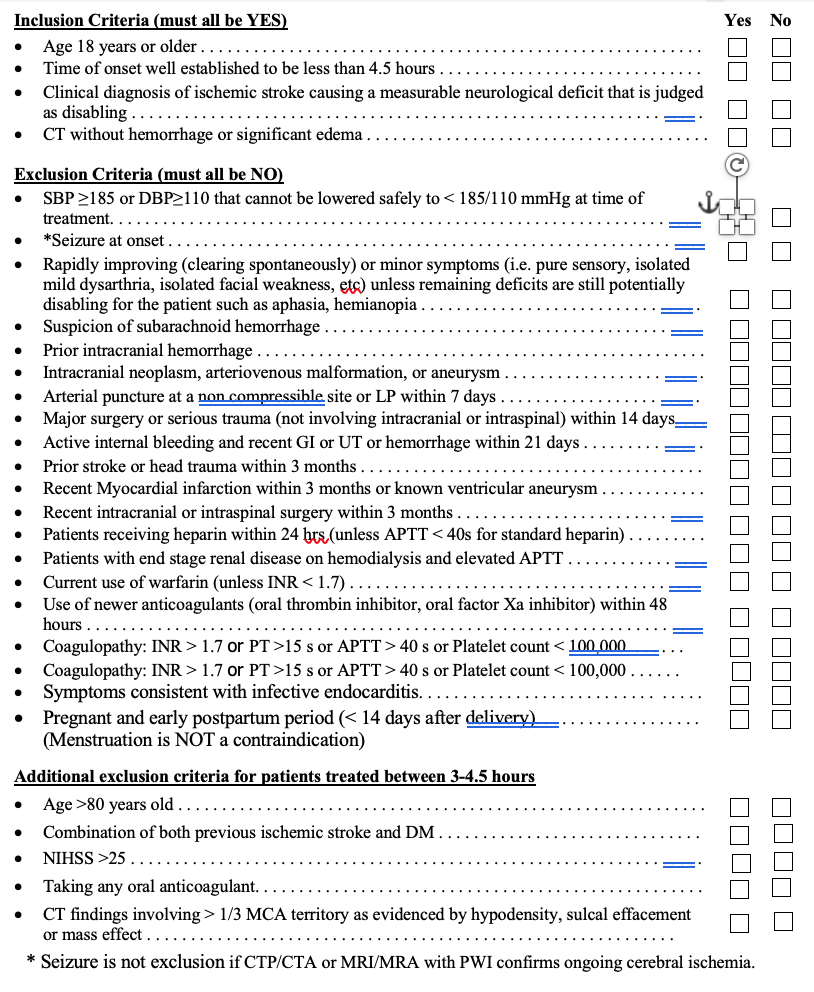
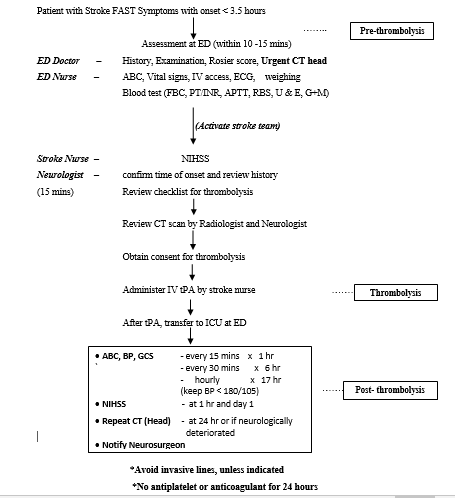
Figure 1. Workflow for Acute Stroke Management Protocol for Administering of tPA
Author Information
Ohnmar, Zarni Myint Shwe, Khin Myat Po Po Kyaw, Phyu Phyu Lay
- Associate Professor, Department of Neurology, University of Medicine 1
- Senior Consultant Neurologist, Department of Neurology, Yangon General Hospital
- Senior Consultant Neurologist, Department of Neurology, Yangon General Hospital
- Professor/Head, Department of Neurology, Yangon General Hospital