Abstract
Achalasia cardia is an oesophageal motility disorder characterized by aberrant peristalsis and insufficient relaxation of the lower oesophageal sphincter. Patients most commonly present with dysphagia to solids and liquids, regurgitation, and occasional chest pain with or without weight loss. As there is no aetiological treatment, different pharmacological agents and invasive techniques have been used for relieving the symptoms. For the past decade, peroral endoscopic myotomy (POEM) has proven to have excellent results.
Three cases that underwent POEM for primary achalasia were presented. Posterior approach for submucosal tunneling was used in these cases. The procedure showed immediate excellent results and no adverse event. We have been following just for 3 months now.
The advantages and disadvantages of POEM compared to the pneumatic dilatation and the Heller myotomy have been extensively studied. Although POEM has become the best for Type 3 achalasia, there is still no universal opinion on which procedure should be the first line treatment in Type 1 and Type 2. The choice of treatment modality depends on institutional strength and patient preference.
Introduction
Achalasia is a motility disorder with yet undiscovered aetiology that is thought to be either viral, autoimmune or neurodegenerative.1 The incidence of achalasia is 1.63/100,000; therefore, it is considered a rare disease.2 It results from progressive degeneration of ganglion cells in the myenteric plexus in the oesophageal wall, leading to failure of relaxation of the lower oesophageal sphincter (LES).3 Thus, the proposed treatments aim to reduce the pressure of LES, namely pharmacologic agents, pneumatic dilation and endoscopic and surgical myotomy.1
Per oral endoscopic myotomy (POEM) represents a natural orifice endoscopic surgical technique for the treatment of achalasia. It utilizes a submucosal tunnel approach that offsets the mucosal and muscle incisions and thus allows secure closure with a few clips on the mucosotomy site.5 Since the introduction of POEM by Inoue and colleagues in 2009, multiple studies have established the safety and efficacy of POEM in achalasia cardia and other non-achalasia spastic oesophageal motility disorders.6 POEM is considered as one of the frontline treatment modalities for the management of achalasia.4, 7, 8
Patients and methods
We performed POEM on three patients with primary achalasia; a 59 year old male (patient A), 36-year-old female (patient B) and a 52-year-old male (patient C). All of them had symptoms of dysphagia and retrosternal pain, as well as weight loss. Patient C had undergone Heller’s cardiomyotomy with fundoplication 10 years ago. Their symptoms were graded according to the Eckardt scoring system (Table 1).9 The patients were diagnosed via barium swallow (except in patient C), upper digestive endoscopy and high resolution manometry (HRM). Patient C had sigmoid a shaped oesophagus and severe mucosal thickening. According to Chicago classification of oesophageal manometry (v3.0), the patients A & C had type 1 achalasia and patient B had type 2 achalasia. 10
With valid informed consents, the procedures were performed in supine position under general anesthesia. A forward-viewing endoscope with a transparent distal cap was used. The distance between the dentition and the cardia of each subject was measured. After injecting normal saline mixed with Indigo Carmine, linear incision was positioned on the posterior wall of the oesophagus, approximately at 5 o’clock, between eight and ten centimeters proximal of the gastroesophageal junction (GEJ). Submucosal tunnel was created from there to 2-3 cm distal of the GEJ (until seeing the second penetrating vessel), onto the gastric side. Once the submucosal tunnel was completed, selective circular muscle myotomy was started from 1-2 cm below downwards and full-thickness myotomy of the lower esophageal sphincter was performed, followed by 2-3cm myotomy into the gastric side. The tunnel was sealed with endoclips only after the relaxation of the LES was verified. On the following day, liquid diet was allowed for both patients. Semisolid diet was then allowed for 7 days before initiation of full diet.
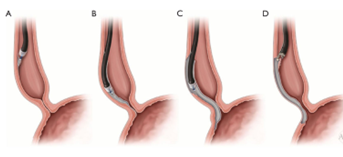
(A) Mucosotomy. (B) Submucosal tunnel. (C) Myotomy. (D) Closure of the mucosotomy
Fig.1 – Steps of POEM procedure 11
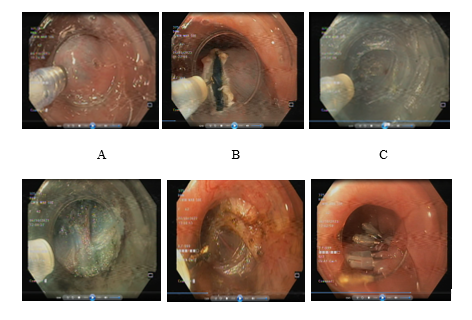
(A) Mucosal lifting (B) Mucosotomy (C)Submucosal tunneling (D) End of tunnel- 2nd penetrating vessel (E) Myotomy (F) Closure of Mucosotomy Site
Fig.2- Endoscopic images of POEM procedure
Results
There were no major adverse events in the intra-operative and immediate post-operative period in all cases. Patient B had mild reflux symptoms (GerdQ 5/18). Their symptoms, if any, were once again graded according to the Eckardt system. The comparison between the pre-procedural and post-procedural score showed excellent results in relieving the symptoms and significant weight gains (Table 2). Barium swallow at one month post-operation revealed significant reduction in stasis and free flow of barium across GEJ (Figures 3 & 4).
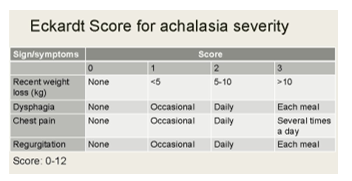
Table.1-Eckardt Score9
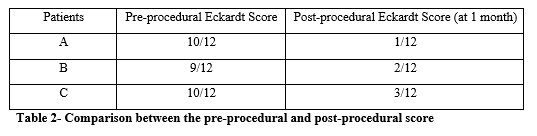
Table 2- Comparison between the pre-procedural and post-procedural score
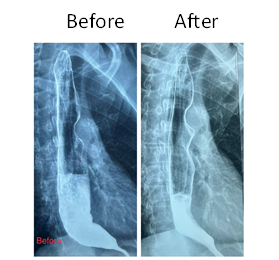
Fig. 3- Pre-procedural and 1 month post-procedural barium study of Patient A
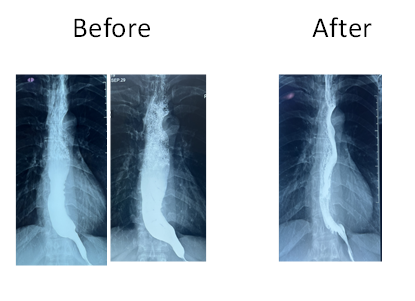
Fig.4- Pre-procedural and 1 month post-procedural barium study of Patient B
Discussion
There are various treatment modalities available for the treatment of achalasia including pharmacotherapy (calcium channel blockers, nitrates, 5-phosphodiesterase inhibitors), botulinum toxin (Botox) injection, PBD and surgical open or laparoscopic myotomy.12 Of these available treatment modalities, the most commonly used are PBD and LHM, which have been proven to have similar therapeutic results at 2 and 5 year follow up.13
The POEM procedure was first performed on humans in 2008 by Inoue et al.6 Since then, it has gained widespread acceptance for the treatment of achalasia. The practical advantage of POEM is that, by avoiding body wall trauma and extensive dissection of the oesophageal hiatus, the procedure is mostly pain-free and allows patients to resume normal activities a couple of days after the procedure.14 Multiple studies from India have demonstrated the excellent safety profile of POEM with significant relief of symptoms, reduction of LES pressure and improvement of oesophageal emptying. 7,8 Capnoperitoneum and submucosal emphysema are inevitable parts of the procedure which can be recognized during the procedure and be easily managed if clinically significant.15
Several studies and meta-analyses have compared the outcomes of POEM to LMH.16 In a randomized controlled trial, comparing POEM to LMH, clinical success at the two years follow-up was observed at 83% of the POEM group and at 81.7% of the surgical myotomy group. When compared, serious adverse events occurred in 2.7% of the subjects after the POEM and in 7.3% after the LMH.[17] POEM provides a distinct advantage over LHM in managing type III achalasia.[18] These patients require longer oesophageal myotomy which can be easily accomplished during POEM. Another advantage of POEM is that it can be done with a reasonable success rate in patients who have undergone previous endoscopic or surgical procedures. 19,20,21
Moreover, when measuring clinical outcomes of POEM and pneumatic balloon dilatation (PBD), the second most used endoscopic technique for treatment of achalasia, the patients that underwent POEM showed significantly better short- and long-term outcomes. 22
Since fundoplication is not performed along with POEM, as it is with Heller myotomy, the development of gastroesophageal reflux disease has been a major concern. Although the incidence of GERD is high after POEM, most of the reflux esophagitis is mild and responsive to PPI therapy.23,24
In conclusion, POEM is a safe, minimally-invasive procedure that shows excellent clinical outcomes and symptoms reduction when used for the treatment of achalasia. It can be used as one of the primary modalities of treatment for achalasia along with LHM and PBD.
References
- Patel DA, Kim HP, Zifodya JS, et al. 2015 “ Idiopathic (primary) achalasia: a review.” Orphanet J Rare Dis; 10:89.
- Sadowski DC, Ackah F, Jiang B, et al. 2010 “ Achalasia: incidence, prevalence and survival. A population-based study”. Neurogastroenterol Motil; 22(9):e256-61.
- Ghoshal UC, Daschakraborty SB, Singh R. 2012 “Pathogenesis of achalasia cardia.” World J Gastroenterol; 18(24):3050–7.
- Jawaid S, Draganov PV, Yang D. 2020 “Esophageal POEM: the new standard of care”. Transl Gastroenterol Hepatol; 5:47.
- Stavropoulos SN, Iqbal S, Modayil R and Dejesus D. 2012 “Peroral endoscopic myotomy, equipment and technique: A step-by-step explanation.” Video J and Encyclopedia of GI Endoscopy; doi: 10.1016/S2212-0971(13)70043-8
- Inoue, H.; Minami, H.; Satodate, H.; Kudo, S. 2009 “First Clinical Experience of Submucosal Endoscopic Myotomy for Esophageal Achalasia with No Skin Incision.” Endosc. 69(5), AB122.
- Ramchandani M, Nageshwar Reddy D, Darisetty S, et al. 2016 “Peroral endoscopic myotomy for achalasia cardia: treatment analysis and follow up of over 200 consecutive patients at a single center.” Dig Endosc.;28:19–26
- Santosh Darisetty, Zaheer Nabi, Mohan Ramchandani, Radhika Chavan, Rama Kotla, D. Nageshwar Reddy, Anesthesia in per-oral endoscopic myotomy: 2017 “A large tertiary care centre experience”, Indian Journal of Gastroenterology, 10.1007/s12664-017-0782-0, 36, 4, (305-312)
- Eckardt, A. J. & Eckardt, V. F. 2011 “Treatment and surveillance strategies in Achalasia: an update”. Rev. Gastroenterol. Hepatol. 8, 311–319
- Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE; . 2014 “International High Resolution Manometry W”orking Group. The Chicago Classification of esophageal motility disorders,” Neurogastroenterol Motil. Feb;27(2):160-74. doi: 10.1111/nmo.12477. Epub PMID: 25469569; PMCID: PMC4308501.
- Petrov RV, Fajardo RA, Bakhos CT and Abbas AE. 2021 “Peroral endoscopic myotomy: Techniques and outcomes.” Shanghai Chest. doi:10.21037/shc.2020.02.02.
- Vaezi MF, Pandolfino JE, Vela MF. 2013 “clinical guideline: Diagnosis and management of achalasia.” Am. J. Gastroenterol.108: 1238–49.
- Boeckxstaens GE, Annese V, des Varannes SBet al. 2011 “Pneumatic dilation versus laparoscopic Heller’s myotomy for idiopathic achalasia.” N Engl J Med. 364: 1807–16.
- Simić AP, Radovanović NS, Skrobić OM, Raznatović ZJ, Pesko PM. 2010 “Significance of limited hiatal dissection in surgery for achalasia”. Gastrointest. Surg; 14: 587–93.
- Yang S, Zeng MS, Zhang ZY, Zhang HL, Liang L, Zhang XW.2014 “ Pneumomediastinum and pneumoperitoneum on computed tomography after peroral endoscopic myotomy (POEM): Postoperative changes or complications?”Acta Radiol.
- Onimaru M, Inoue H, Fujiyoshi Y, et al. 2021 “Long-term clinical results of per-oral endoscopic myotomy (POEM) for achalasia: First report of more than 10-year patient experience as assessed with a questionnaire-based survey.” Endosc Int Open; 9(3):E409–E416.
- Werner YB, Hakanson B, Martinek J, et al.2019 “Endoscopic or surgical myotomy in patients with idiopathic achalasia”. N Engl J Med; 381(23):2219–29.
- Sharata AM, Dunst CM, Pescarus Ret al. 2015 “Peroral Endoscopic Myotomy (POEM) for Esophageal Primary Motility Disorders: Analysis of 100 Consecutive Patients”. Gastrointest. Surg; 19(1): 161–70.
- Orenstein SB, Raigani S, Wu YVet al. 2015 “Peroral endoscopic myotomy (POEM) leads to similar results in patients with and without prior endoscopic or surgical therapy”. Endosc.; 29(5): 1064–70.
- Onimaru M, Inoue H, Ikeda Het al. 2013 “Peroral endoscopic myotomy is a viable option for failed surgical esophagocardiomyotomy instead of redo surgical Heller myotomy: a single center prospective study”. Am. Coll. Surg; 217: 598–605.
- Nabi Z, Ramchandani M, Chavan R, Tandan M, Kalapala R, Darisetty S, Lakhtakia S, Rao GV, Reddy DN. 2018 “Peroral endoscopic myotomy in treatment-naïve achalasia patients versus prior treatment failure cases.” Endoscopy. 50(4):358-370.
- Ofosu A, Mohan BP, Ichkhanian Y, et al. 2021 “Peroral endoscopic myotomy (POEM) vs. pneumatic dilation (PD) in treatment of achalasia: A meta-analysis of studies with ≥ 12-month follow-up.” Endosc Int Open; 9(7):E1097–E1107.
- Facciorusso A, Singh S, Abbas Fehmi SM, et al.2021 “Comparative efficacy of first-line therapeutic interventions for achalasia: a systematic review and network meta-analysis”. Surg Endosc 35(8):4305–14.
- Nabi Z, Ramchandani M, Kotla R, Tandan M, Goud R, Darisetty S, Rao GV, Reddy DN. 2020 “Gastroesophageal reflux disease after peroral endoscopic myotomy is unpredictable, but responsive to proton pump inhibitor therapy: a large, single-center study.” Endoscopy.52(8):643-651.
Author Information
Linn Htet Oo, Than Than Aye, Zeyar Lwin, Tin Moe Wai, Swe Mon Mya, Moe Myint Aung, Thein Myint, Than Than Aye, Zaheer Nabi
- Consultant Gastroenterologist , Department of Gastroenterology, Yangon General Hospital
- Associate Professor, Department of Gastroenterology, Yangon General Hospital
- Professor, Department of Gastroenterology, University of Medicine (2),Yangon
- Professor, Director of WGO Myanmar Training Center, Patron of Myanmar GI & Liver Society
- Professor & Head, Department of Gastroenterology, University of Medicine(1),Yangon General Hospital, President of Myanmar GI & Liver Society
- Senior Consultant Gastroenterologist and Clinical Director of Interventional Endoscopy, Department of Gastroenterology, Asian Institute of Gastroenterology, Hyderabad , India