
Constipation is a chronic problem in many patients all over the world. Constipation is a common complaint that may be primary (idiopathic or functional) or associated with a number of disorders or medications. It can be mild and transitory, or chronic and unresponsive to treatment, and is more prevalent and more severe in women. Constipation that is refractory to available laxatives should be evaluated for defecatory disorders and slow-transit constipation using studies of anorectal function and colonic transit.1
Definition and classification of constipation
Constipation is defined by bowel disturbances (ie, reduced frequency of bowel movements, hard stools, excessive straining to defecate, a sense of anorectal blockage, anal digitation, and a sense of incomplete evacuation after defecation).2
Constipation can be divided into two groups. Primary constipation results from disordered regulation of colonic and anorectal neuromuscular function as well as brain–gut neuroenteric functions. Secondary constipation results from a plethora of factors that include diet, drugs, behavioral, endocrine, metabolic, neurological, and other disorders.2
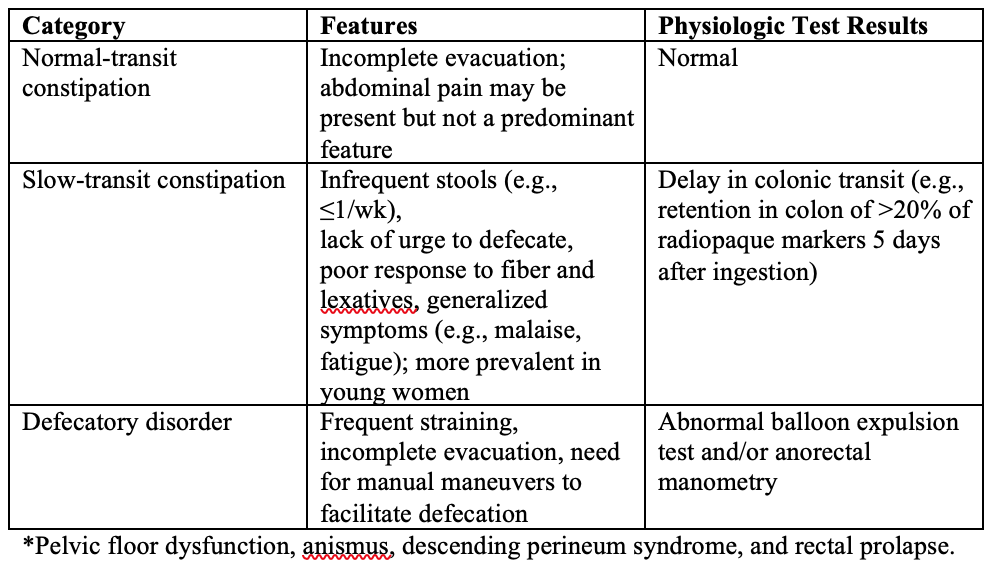
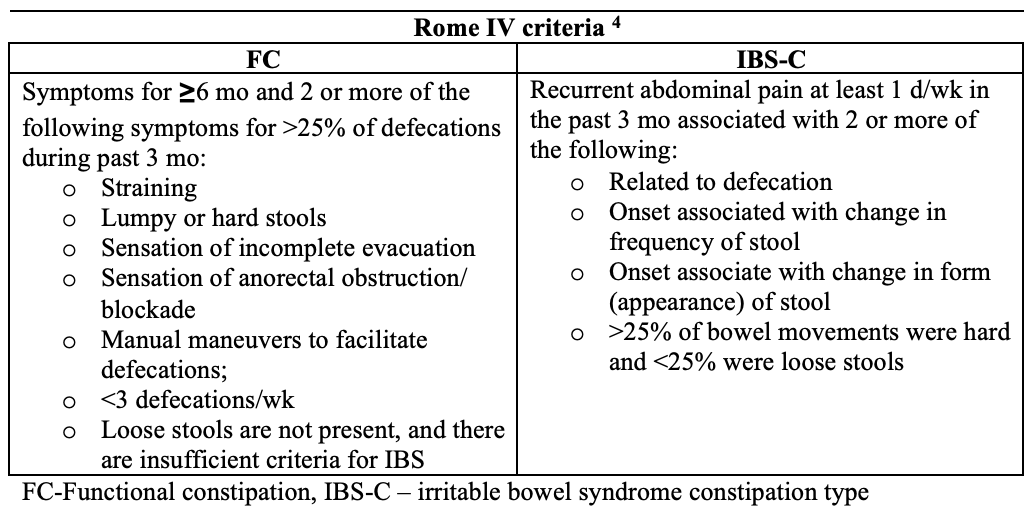
There are two approaches for classifying chronic constipation. The American Gastroenterological Association criteria utilize colonic transit and anorectal tests to classify constipated patients into 1 of 3 groups: normal- transit constipation (NTC), slow-transit constipation (STC), and pelvic floor dysfunction or defecatory disorders (DD). 2 Clinicians frequently assess colonic transit and anorectal functions in constipated patients who have not responded to pharmacotherapy. By contrast, epidemiological studies and pharmaceutical trials use the original, or suitably modified, so-called Rome criteria (the most recent iteration is the Rome IV criteria), which incorporate symptoms and anorectal assessments of rectal evacuation.3
Clinical classification of functional constipation1
Risk factors
Increasing age, female sex, lower socioeco- nomic status, lower parental education rates, less self-reported physical activity, certain medications, stressful life events, physical and sexual abuse, and depression are associated with constipation.1
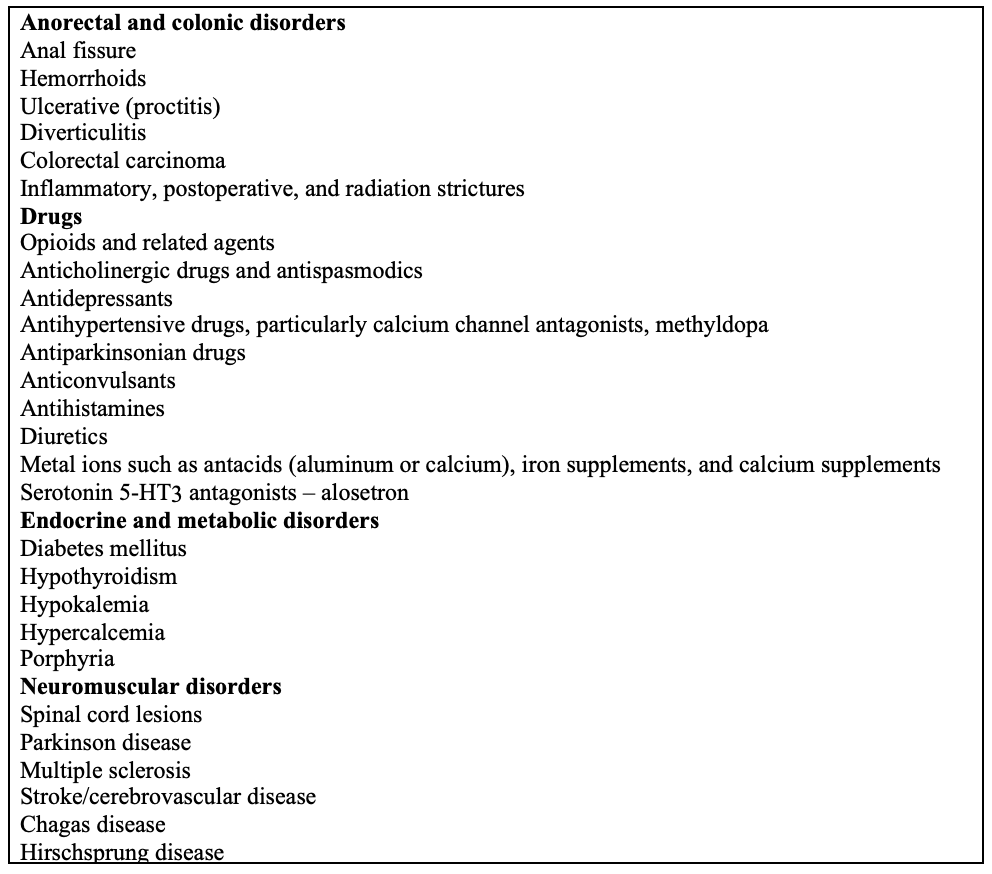
Common causes of secondary constipation1
Clinical evaluation of chronic constipation6
Medical history
A detailed medical, surgical, and drug history can help to identify most organic and secondary causes of constipation.
The medical history and physical examination in constipation patients should focus on identifying possible causative conditions and alarm symptoms.
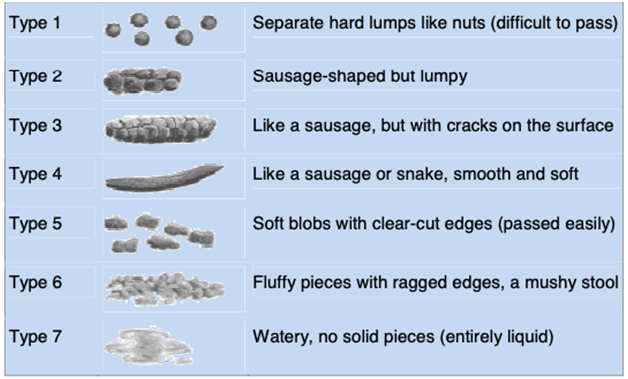
- Stool consistency. This is regarded as a better indicator of colon transit than stool frequency
The Bristol Stool Form Scale: a measure to assist patients in reporting on stool consistency 5
- Patient’s description of constipation symptoms; symptom diary: — Bloating, pain, malaise
- Nature of stools
- Bowel movements
- Prolonged/excessive straining
- Unsatisfactory defecation
- Laxative use, past and present; frequency and dosage
- Current conditions, medical history, recent surgery, psychiatric illness
- Patient’s lifestyle, dietary fibre, and fluid intake
- Use of suppositories or enemas, other medications (prescription or over-the-counter)
- Physical examination:
- Gastrointestinal mass
- Anorectal inspection:
- Fecal impaction
- Stricture, rectal prolapse, rectocele
- Paradoxical or nonrelaxing puborectalis activity
- Rectal mass
- If indicated: blood tests—biochemical profile, complete blood count, calcium, glucose, and thyroid function
Alarm symptoms 6
- Change in stool caliber
- Heme-positive stool
- Iron-deficiency anemia
- Obstructive symptoms
- Patients > 50 years with no previous colon cancer screening
- Recent onset of constipation
- Rectal bleeding
- Rectal prolapse
- Weight loss
Diagnostic Tests
Further diagnostic testing is unnecessary for most patients who complain of mild symptoms, especially adolescents, young adults, and those without alarm features. Investigations may be indicated for 1 of 2 reasons: (a) to exclude a systemic illness or structural disorder of the GI tract as a cause of constipation or (b) to elucidate the underlying pathophysiologic process when symptoms are unresponsive to simple treatment.1
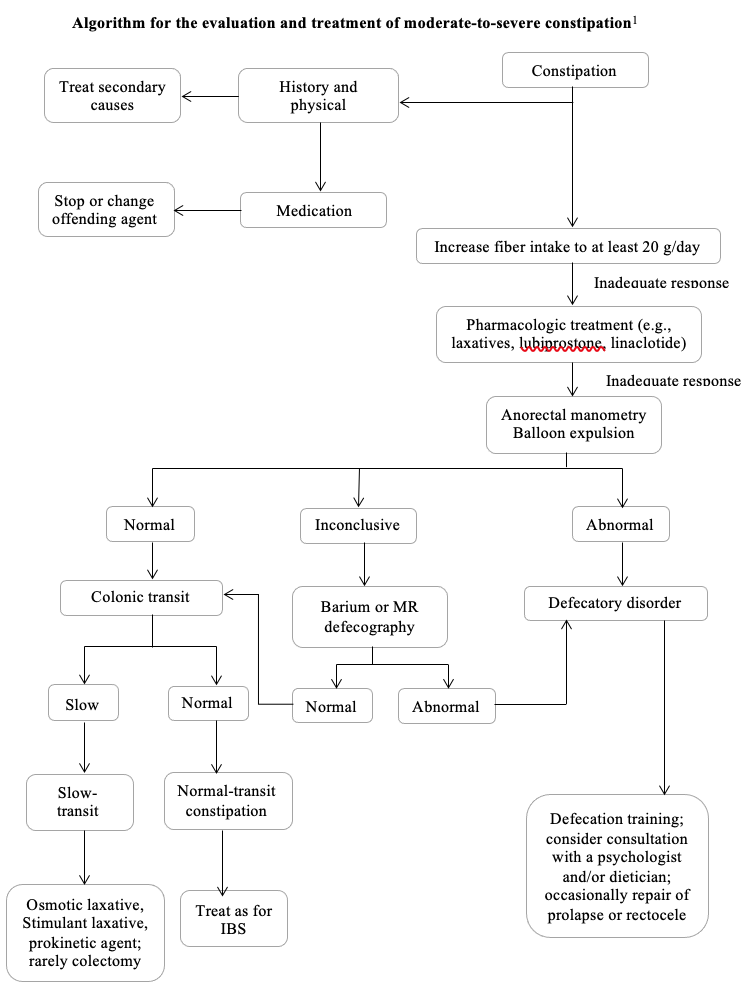
Anorectal testing with manometry and balloon expulsion test are recommended for patients who have not responded to a high-fiber diet and/or simple laxatives. Because access to ano- rectal testing is not universal, some practitioners treat patients empirically with prescription laxatives before anorectal testing.1
Tests for Systemic Disease
Determination of the hemoglobin level, ESR, and biochemical screening test levels (e.g., thyroid function, serum calcium, glucose, and other appropriate investigations) are indicated if the clinical picture suggests that symptoms may be due to an inflammatory, neoplastic, metabolic, or other systemic disorder.7
Tests for Structural Disease
Imaging of the colon by a CT, MRI, or barium enema study reveals the width and length of the colon and may be indicated to exclude an obstructing lesion severe enough to cause constipation. A colonoscopy is recommended only when there has been a recent change in bowel habits, blood in the stool, or other alarm symptoms.8
Physiologic Measurements
Physiologic testing is reserved for patients with refractory symptoms. Testing can be performed to measure colonic transit time, evaluate pelvic floor functioning during defecation, and exclude anatomic abnormalities that could cause constipation.6
Colonic Transit Time
Studies that measure colonic transit time are important for confirming and quantifying a patient’s complaint of constipation and identifying slow transit and regional delay. Colonic transit can be assessed by using radiopaque markers, colon scintigraphy, colonic manometry, or the wireless motility capsule, only when indicated after anorectal testing, and after discontinuing medications that can affect colonic transit.2
Balloon Expulsion Test
The balloon expulsion test can suggest a defecatory disorder in a patient with no or delayed evacuation of a 50-mL water-filled balloon from the rectum; the test is generally performed while the patient is sitting on a commode. 2
Anorectal Manometry
Anorectal manometry can assess the resting and maximum squeeze pressures of the anal sphincters, presence or absence of relaxation of the anal sphincter during balloon distention of the rectum (rectoanal inhibitory reflex), rectal sensation, and ability of the anal sphincter to relax during straining.1
Defecography
Defecography evaluates the rate and completeness of rectal emptying, anorectal angle, and amount of perineal descent and identifies structural abnormalities (e.g., large rectocele, internal mucosal prolapse, intussusception). 2
Management of Chronic Constipation
Nonpharmacologic Management
Nonpharmacologic treatment is the first-line management in constipation. This approach relies on educating patients about diet, fiber and fluid intake, physical activity, and toilet training.
Dietary fibers are carbohydrate polymers and are digested in small extant in the colon. They may be soluble and insoluble, whereas soluble fibers are more effective. One of the most often recommended is Psyllium. In the treatment of constipation, the recommendation is to gradually increase fiber intake, to a maximum of 35 g per day. Not all patients with constipation respond to treatment with fiber, the exceptions are patients with refractory constipation, slow transit constipation, or dyssynergic defecation.9
Physical activity has positive influence on patients, moderate to vigorous activity alleviates symptoms and improves the quality of life in IBS.2
Treating constipation with increased fluid intake is only effective in dehydrated patients and poor water consumption is not associated with a higher risk of evacuation disorders.11
Biofeedback therapy is especially effective in patients with defecatory disorders. The main purpose of this treatment is to restore normal pattern of defecation and to correct dyssynergia between abdominal, rectal, and anal sphincter muscles, and to increase rectal perception.3
Pharmacological Management
(1). Laxatives
Laxatives, due to their effectiveness and availability, are the most commonly used pharmaceuticals in constipation. In case of failure of nonpharmacological management, laxatives are the first line of medications.10
Osmotic laxatives change osmotic gradient in the intestine. As a result, secretion of water and electrolytes in the intestine is higher, ultimately volume of stool is increased and consistency is reduced. They are usually well tolerated in long term use. One of the commonly used osmotic laxatives is polyethylene glycol (PEG). Recommended dose of PEG per day is 10–20 g. Lactulose, as well as PEG, is an osmotic laxative. 10
Saline laxatives, like magnesium citrate and sulfate (Ebson salt), disodium phosphate, sodium phosphate which transport water to the lumen of small and large intestine, also belong to the group of osmotic laxatives. Saline laxatives should be carefully considered in elderly patients or at risk of cardiovascular diseases, renal impairment, and hypertension. 11
Another group are stimulant laxatives that directly stimulate intestinal motility by Auerbach and myenteric plexus, and increase water and electrolyte secretion to the intestinal lumen.
Stimulant laxatives are usually prescribed as the next step in the management of functional constipation. The common examples of this group are sodium picosulfate, senna and cascara (both present in teas), and the most popular bisacodyl.12
(2). Secretagogues (Lubiprostone, Linaclotide)
Prosecretory agents treat constipation by modulating ion channels of epithelium to enhance colonic secretion and improve colonic transit.13
(3). Serotoninergic Agonists (Prucalopride, Velusetrag)
Serotonin agonists, by activating 5-hydroxytryptamine receptor 4 (5-HT4) located in the gastrointestinal tract, stimulate secretion of the intestine and its motility. 13
(4). Probiotics and Prebiotics
Various probiotic species and strains have been suggested as beneficial agents regarding gastrointestinal diseases and gut motility. Many studies confirmed their effectiveness in adult patients with constipation, based on improvement in intestinal transit and stool consistency, increased evacuation frequency, and decreased flatulence.14 Moreover, studies showed that the effects of probiotics are species- and strain-specific, with indication that multispecies strains with Bifidobacterium lactis have the most promising beneficial effects. 1
Surgical Approach
Patients with slow-transit constipation may be treated with ileostomy, total colectomy with ileorectal anastomosis (after removal of the colon, the ileum is connected to rectum), cecostomy with antegrade enemas. Patients with outlet rectal obstruction syndrome mostly require repair of rectoceles or surgery for rectal intussusception. Those with combination of dyssynergic defecation and slow-transit constipation may benefit from a segmental colonic resection or total colectomy, but pelvic floor dysfunction should be corrected first. Ileostomy is a surgical intervention that may relieve uncorrectable, severe pelvic floor dysfunctions.8
Other Possibilities of Treatment
(a). Acupuncture
Acupuncture and electro-acupuncture is Chinese treatment modality. Patients with severe constipation may be treated with acupuncture, however they should not have any comorbidities, and their constipation should not be caused by medications. 10
(b). Fecal Microbiota Transplantation (FMT)
Owing to dysbiosis of gut microbiota being a possible cause of constipation, FMT was suggested to be a method of treatment.1
(c). Massage
An alternative, but also effective nonpharmacological method, is abdominal massage. According to Sinclair, abdominal massage may accelerate colonic transit time, stimulate peristalsis and lower the pain and discomfort that often occur with constipation.13
References
- Johanna C. Iturrino, Anthony J. Lembo, (2021) Constipation,Sleisenger and Fordtran’s Gastroenterology and Liver Disease (11th edition), pg 250-273
- Bharucha, A.E.&Wald, A. (2019) Chronic Constipation. Mayo Clin. Proc., 94, 2340–2357.
- Rao, S.S, Bharucha A.E, Chiarioni G, et al. (2016) Functional anorectal disorders.Gastroenterology. 150(6):1430-1442.e4.
- Bharucha, A.E&Lacy,B.E. (2020) Mechanisms, Evaluation, and Management of Chronic Constipation. Gastroenterology; 158:1232–1249
- Costilla, V.C.; Foxx-Orenstein, A.E. (2014) Constipation. Understanding Mechanisms and Management. Clin. Geriatr. Med; 30, 107–115.
- GregerL, Saeed H et al, (2010) Constipation:a global perspective, World Gastroenterology Organisation Global Guidelines; pg 1-13
- Pannemans, J. Masuy, I. Tack, J. (2020) Functional Constipation: Individualising Assessment and Treatment. Drugs, 80, 947–963.
- Włodarczyk. J, Anna W.N, Jakub F, Adam D, Łukasz D and Marcin W, (2021) Current Overview on Clinical Management of Chronic Constipation.J. Clin. Med, 10, 1738
- Eswaran. S, Muir. J. Chey, W.D. (2013) Fiber and functional gastrointestinal disorders. Am. J. Gastroenterol. 108, 718–727.
- Lee, H.Y. Kwon, O.J. Kim, J.E; Kim, M. A.R.Park, H.-J. Cho, J.-H. Kim, J.H. Choi, S.M. (2018) Efficacy and safety of acupuncture for functional constipation: A randomised, sham-controlled pilot trial. BMC Complement. Altern.Med. 18, 186.
- Dupont, C. Hébert, G. (2020) Magnesium Sulfate-Rich Natural Mineral Waters in the Treatment of Functional Constipation—A Review. Nutrients, 12, 2052.
- Irwin, K. (2007) Laxatives. In Therapeutic Management of Incontinence and Pelvic Pain: Pelvic Organ Disorders; Springer: London, UK; pp. 227–230.
- Choi, Y.I. Kim, K.O. Chung, J.W. Kwon, K.A. Kim, Y.J. Kim, J.H. Park, D.K. (2020) Effects of Automatic Abdominal Massage Device in Treatment of Chronic Constipation Patients: A Prospective Study. Dig. Dis. Sci. 3105-3112.
- Zhang, C. Jiang, J. Tian, F. Zhao, J. Zhang, H. Zhai, Q. Chen, W. (2020) Meta-analysis of randomized controlled trials of the effects of probiotics on functional constipation in adults. Clin. Nutr. 39, 2960–2969.
- Dimidi, E,Christodoulides, S, Fragkos, K.C, Scott, S.M, Whelan, K, (2014) The effect of probiotics on functional constipation in adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 100, 1075–1084.
Author Information
Thein Myint1, Sandar Win2
- Professor/ Head (retired), Department of Gastroenterology, Yangon General Hospital
- Associate professor, Department of Gastroenterology, University of Medicine (1), Yangon General Hospital

