We report a case of pancreatic fistula in a 26 year old man living in Pyay and discuss the implications for diagnostic testing and treatment for pancreatic fistula.
Case Report
A 26 year old man from Pyay was referred from surgical ward, New Yangon General Hospital (NYGH) to our GI ward on August 2018 for pancreatic fistula. According to clinical history, he suffered abdominal pain off and on for one year duration. In January, 2018, the pain became more severe for one week. That occurred in epigastrium and left upper abdomen, which was radiated to back. There were no aggravating or relieving factors. Apart from the abdominal pain, he denied any symptoms such as nausea, vomiting, hemetamesis & melaena, bleeding per rectum, loss of appetite, loss of weight, fever and other systemic symptoms.
He had a consultation at a Private hospital, Pyay and an abdominal USG was done and it revealed a splenic abscess. He underwent an operation at that private hospital and was referred to thesurgical ward, New Yangon General Hospital for further management on the second post operative day.
On arriving to the Surgical ward, NYGH, the patient’ vital signs were stable and there was a surgical scar and an external drainage tube at LHC. Investigations done included: FBC, Urea, electrolytes, creatinine and imaging (USG abdomen and CT abdomen). They revealed neutrophil leucocytosis and aasplenic abscess with minimal left pleural effusion and chronic pancreatitis.
A second operation was done on 18th January and the pre- operative diagnosis was splenic abscess and left retroperitoneal abscess (lt paracolic gutter) which contained necrotic debris and pus, a splenic haematoma, pancreatic calcification, marked fibrinoid adhesion between stomach, spleen, transverse & descending colon, small intestine and splenectomy and drainage of retroperitoneal abscess at left paracolic gutter and post operative diagnosis was left retroperitoneal abscess.
Investigations after operation (FBC, Urea, creatinine and electrolytes) were within normal limit and showed no fluid collection in USG (abd). Histology report was chronic non specific inflammation, retroperitoneal and congestive splenomegaly. The external drain amount was 50 – 100 cc of clear fluid daily and the amount increased each day in the post-op period. Therefore, pancreatic fistula was suspected and necessary investigations were done to confirm the diagnosis.Serum amylase was 171 U/L and drain fluid amylase was 88300 U/L and CT Abdomen confirmed chronic pancreatitis and post splenectomy abscess.
ERCP was done in GI ward, YGH with the indication of post splenectomy pancreatic fistula. ERCP findings as pancreatic duct were dilated and tortuous at head and body and some narrowing was seen at the body. The following therapeutic procedure was done.Wire guided deep cannulation was done. Contrast was injected into pancreatic tree to make pancreatogram. Pancreatic duct was dilated and tortuous at head and body and some narrowing was seen at body. Pancreatic sphincterotomy was done by sphincterotome. Single pig tail plastic stent 7 Fr x 12 cm was inserted into pancreatic duct.
The external drainage amount was nil since the next day after ERCP. And patient was referred back to surgical ward, NYGH. Removal of external drain was done. Patient attended follow up to GI ward andhad no special complaints and patient’s wellbeing was improved. We plan to remove pancreatic stent in six month.

Before ERCP

One month after ERCP
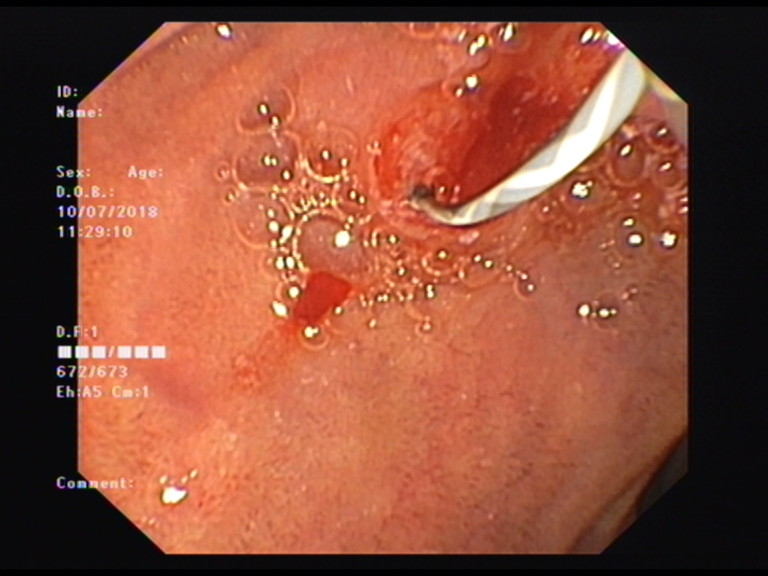
Pancreatic duct cannulation
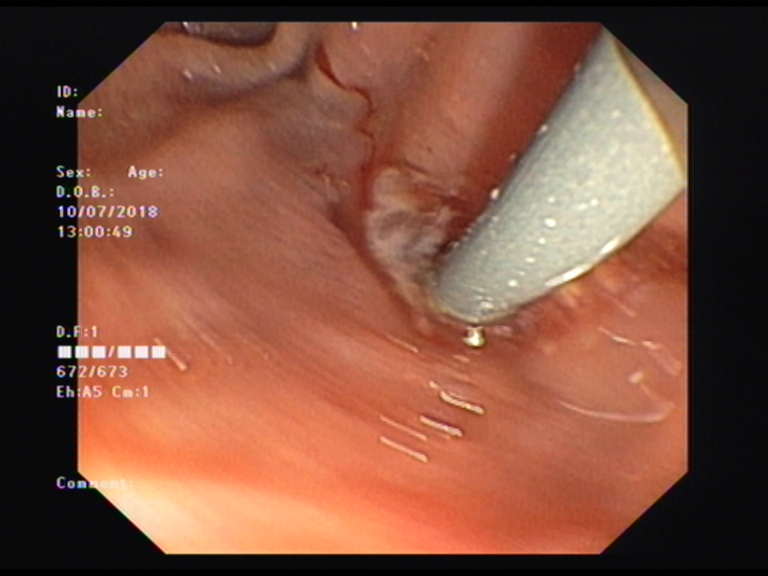
Pancreatic duct dilatation with dilator
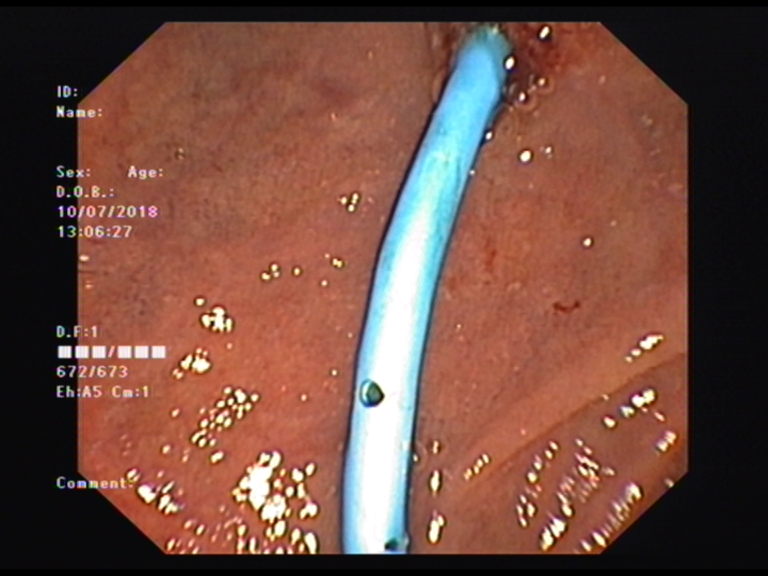
Pancreatic stent insertion
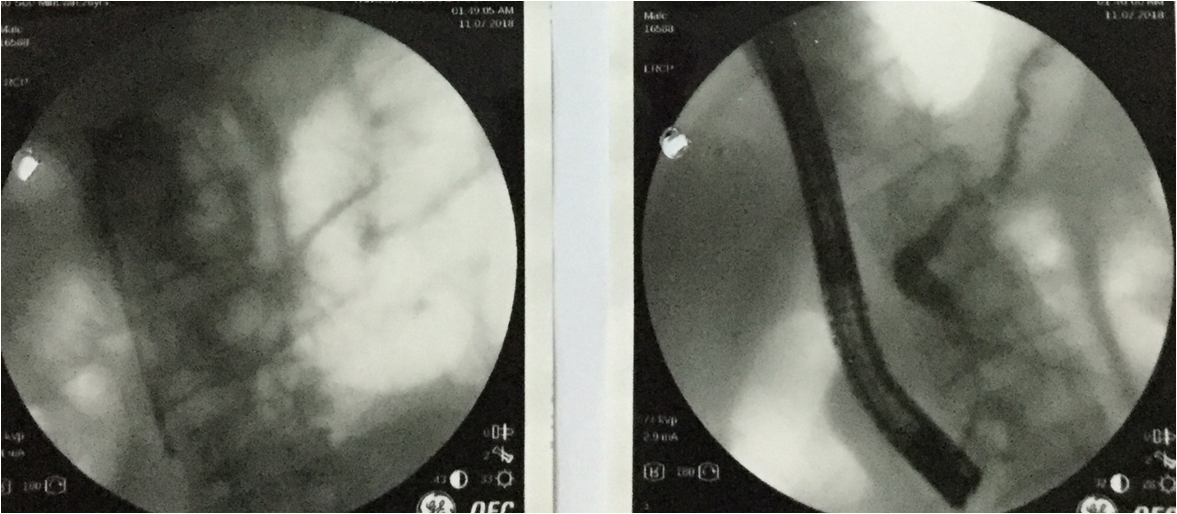
Pancreatogram
Discussion
Pancreatic duct leaks and pancreatic duct disruptions may occur as sequelae of acute or chronic pancreatitis as well as after pancreatic surgery (eg. after distal pancreatectomy) and trauma.7The injury may range from mild to complete transaction resulting in a disconnected pancreatic duct. Pancreatic duct leaks can result in pancreatic ascites, pleural effusion, or early (acute fluid or necrotic collection) or late complications (pseudocyst or walled off necrosis)6 External leaks (pancreatic-cutaneous fistulas) usually occur following pancreatic surgery or percutaneous drainage of pancreatic fluid collections. External fistulae are identified by output of high-amylase fluid.7
The role of ERCP in pancreatic ductal leaks is to place a trans papillary stent into the pancreatic duct, at least across the sphincter and preferably to bridge the area of leak, with resolution reported in three-quarters of patients, depending on a number of factors including whether or not the site of leak could be bridge.6Most pancreatic leaks that occur after pancreatic surgery are already controlled by indwelling surgical drains. Many of these leaks will close over time; endoscopic therapy is generally reserved for persistent or refractory leaks. In the absence of a surgical drain, endoscopic therapy is performed to treat symptomatic leaks.7
In patients with external drains in whom endoscopic therapy is being performed to allow drainage removal.Success depends on the size of the external drain as compared with the size of the internal stent. Downsizing, clamping, or removing the external drain after successful endoscopic stent placement can promote internal drainage and fistula closure.7
References
6. Arain , M. A. and Freeman, M.L. (2016) Endoscopic retrograde cholangiopancreatography. In: Yamada’s Textbook of Gastroenterology, Sixth Edition: pg 2582-2611. John Wiley & Sons, Ltd.
7. Ferreira, L.E. and Baron, T.HFrank K. Friedenberg (2016). Gastroesophageal Reflux Disease In: Sleisenger and Fordtran’s Gastrointestinal and Liver Disease, Tenth Edition : pg 1045-1052. Saunders press.
- Professor and Head, Department of Gastroenterology, Yangon General Hospital
- Professor, Department of Gastroenterology, Yangon General Hospital
- Associate Professor, Department of Gastroenterology, Yangon General Hospital
- Consultant Gastroenterologist, Department of Gastroenterology, Yangon General Hospital
- Doctorate student, Department of Gastroenterology, University of Medicine 1, Yangon
Thein Myint1, Moe Myint Aung2, Tin Moe Wai3, Swe Mon Mya3, Mya Thet Nwe4, Sandar Win4, Thida Soe4, Nang Khin Phone Tint5 Department of Gastroenterology, Yangon General Hospital