Introduction
Many practitioners consider that examination of a child is a difficult task and most of them are reluctant to see a child in their clinics. In a country like Myanmar, where the under fifteen population is 27.8 percent and under five population is 8.7 percent of total population, it is unavoidable, especially in the field of general practice (Myanmar National Census Report 2015). In addition, most parents will bring their children to the clinics even with the minor illnesses, whereas they might not seek medical attention for their illnesses which may be more serious. If a medical practitioner knows the nature of children and some secrets of pediatric clinical examination, he or she will find that pediatric examination is much easier than commonly believed.
The environment
Although adult patients will be impressed by your high standard clinic well equipped with instruments and monitoring machines, the child will be much frightened by these things. These sophisticated equipment must be hidden from their view. The children’s clinic should look more like a playground rather than a hospital or a clinic. In other words, we have to create a “Playground environment”. (Photo 1)

Photo (1) “Playground environment”
Even the name of the wards should be changed, for example instead of calling Ward 22, our children ward is called “Rainbow Unit” in Law Hospital, Scotland. Most of the children hospitals have a playground-like waiting areas in outpatient departments and playroom in each child ward. (Photo 2 – playroom)
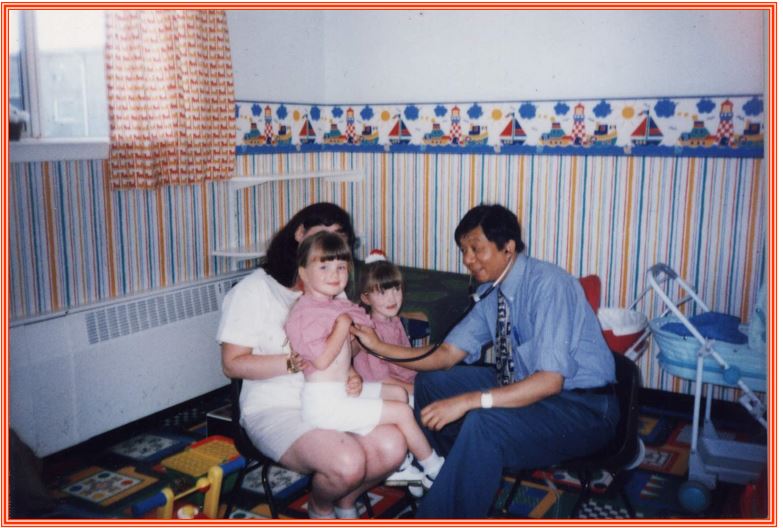
Photo (2) examination of a child in play room of the ward
Toys
Almost all children like and are interested in toys. Therefore toys are essential in dealing with a child. Toys should be age-appropriate for a particular child and it should be safe for him. For example – rattles are for infants, balls for one to three years old and painting cards for above three years. An infant will not understand how to use a toy car and a toddler may purposely swallow a small wheel of it. So that it is really important to select age-appropriate and safe toys for them. Toys should be on your examination area and let the child play with them when you take history from the parents. (Photo 3, 4 )

Photo (3) giving a rattle

Photo (4) building rapport
Be Friendly, Cheerful and Gentle
Children are generally very observant and interested in their surroundings. For them, a smiling person is good and a person with a frown is bad whether your inner nature is good or bad. Please wear a smile on your face whether you are under stress or not. Be friendly to the parents and cheerful to the child. Don’t be annoyed if a child is afraid of you and cry, accept it as a normal phenomenon. To examine a child, you should be very gentle. If a child needs to be undressed, let the parent do it rather than the nurses or yourself.
The Approach Code
b. Stop – The first rules in approaching any child are very similar to those for crossing the road – stop, listen, look and use your other senses. The first approach is a hands-off one- stop. Allow the child to look at you and, insofar as he can, decide you are a person to be trusted. Let him look at you as you talk to the mother. Take your time, make no sudden moves (for you may frighten a fretful toddler) and be in no hurry to examine the child. Even better, let him play in your presence. Approach cautiously, be nice, utter reassuring sounds like brave boy, clever girl etc. (Photo -5)
Photo (5) first thing you have to do
c. Listen – to the mother. Children may come to the clinics accompanied by a variety of care-takers. In our pediatrician’s view, there is no substitute for the mother. She knows her child. The guiding principle in listening is: the mother is usually right until or unless proved otherwise. We have to remember that an observant mother is sometimes more right in assessing her child than a poor doctor. At the same time, you may have the opportunity to listen to the child talk, relate to his mother, and note his breathing, cough and stridor (if present) and other auditory phenomena such as his cry.
d. Look –Look at both mother and child. Is he sick or well? Is he looks normal or abnormal? Does he resemble his parents? Always look at children without staring or looking closely at them. Adequate time should be given for inspection as it is the main part of pediatric examination.
e. Use your other senses – touch, smell and use your stethoscope. The child’s doctor need to be gentle of touch. Mostly we do auscultation before doing the palpation or percussion especially in younger children.
Vital Signs or Energy
The best indications of health in a child is “Energy”. The presence or absence of energy is more important than other vital signs and useful in deciding whether to admit a child or discharge a child admitted in hospital. Always remember to ask about the energy in a child.
Sequence of examination
There are variations in sequence of examination of a child and adults. The usual sequence in examination in adults is – inspection, palpation, percussion and auscultation. But in a child especially in a younger one as toddler, it is better do inspection, auscultation, palpation and percussion. We used to listen to breath or heart sounds first before the child starts to cry.
Concerning the vital signs, these are generally taken by nurses or healthcare assistants before seeing a doctor. But for those children who are not seriously ill it might not be true. Taking vital signs by nurses with limited pediatric experience will make your examination a disaster. So that most of the time, you may see the child first and only required vital signs are asked to taken after that.
Be opportunist and no rigid schedule
You have to take the best opportunity in examination of a child rather than follow a rigid schedule as in examination of an adult. For example, if a child is leaning with his chest on a standing father, you should first listen to breath sounds from the back first. (Photo -6) If a child is sleeping on his back, you can listen to the chest and also palpate abdomen. (Photo- 7) You should not be rigid in both system and examination methods. If the child is screaming, you can look for the tonsils and throat. Remember that a sleeping child is luxury for a pediatrician and must try your best not to wake him up. The child on breastfeeding is usually very calm and easier to examine. So it is a bad mistake to ask to stop feeding for your examination. (Photo– 8). You should do your examination in children’s comfortable preferred position and not yours. (Photo – 9,10,11)

Photo (6) Examination of the back first

Photo (7) Palpation of abdomen in a sleeping child

Photo (8) Examination during breastfeeding

Photo (9) children’s preferred position

Photo (10) child’s preferred position – standing

Photo (11) Patient’s comfortable position 3
Explain or demonstrate
You should explain or demonstrate what you are going to do whenever possible. For example, you can calm down a frightened toddler who is afraid of your stethoscope by listening first to the elder sibling or a doll or on the mother’s arm. If you are going to do any procedure try to explain to parent as well as to the children. If you are going to give an intramuscular or intravenous injection, do not say that it will not be painful. Instead of that, honestly say that it will cause some pain but we will try our best to make it less painful. Parents or caretakers should come along with the child into the procedure room to comfort the child when we do the procedures like intravenous cannula insertion, lumbar puncture or bone marrow aspiration.
Unpleasant procedures last
The doctor should leave the strange or unpleasant procedure to the last part of the examination. Examples of these procedures include blood pressure measurement, throat examination, otoscopic examination and opthalmoscopic examination. Proper holding of the child by mother or caretaker is required for the success of these procedures and the doctor or nurses have to instruct them properly.( Photo–12,13)
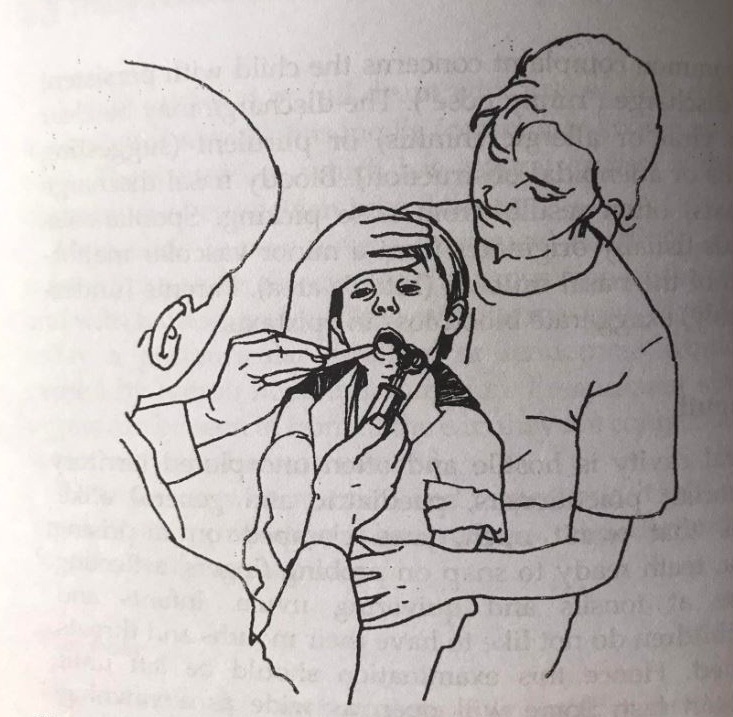
Photo (12) holding a child for examination of mouth and throat
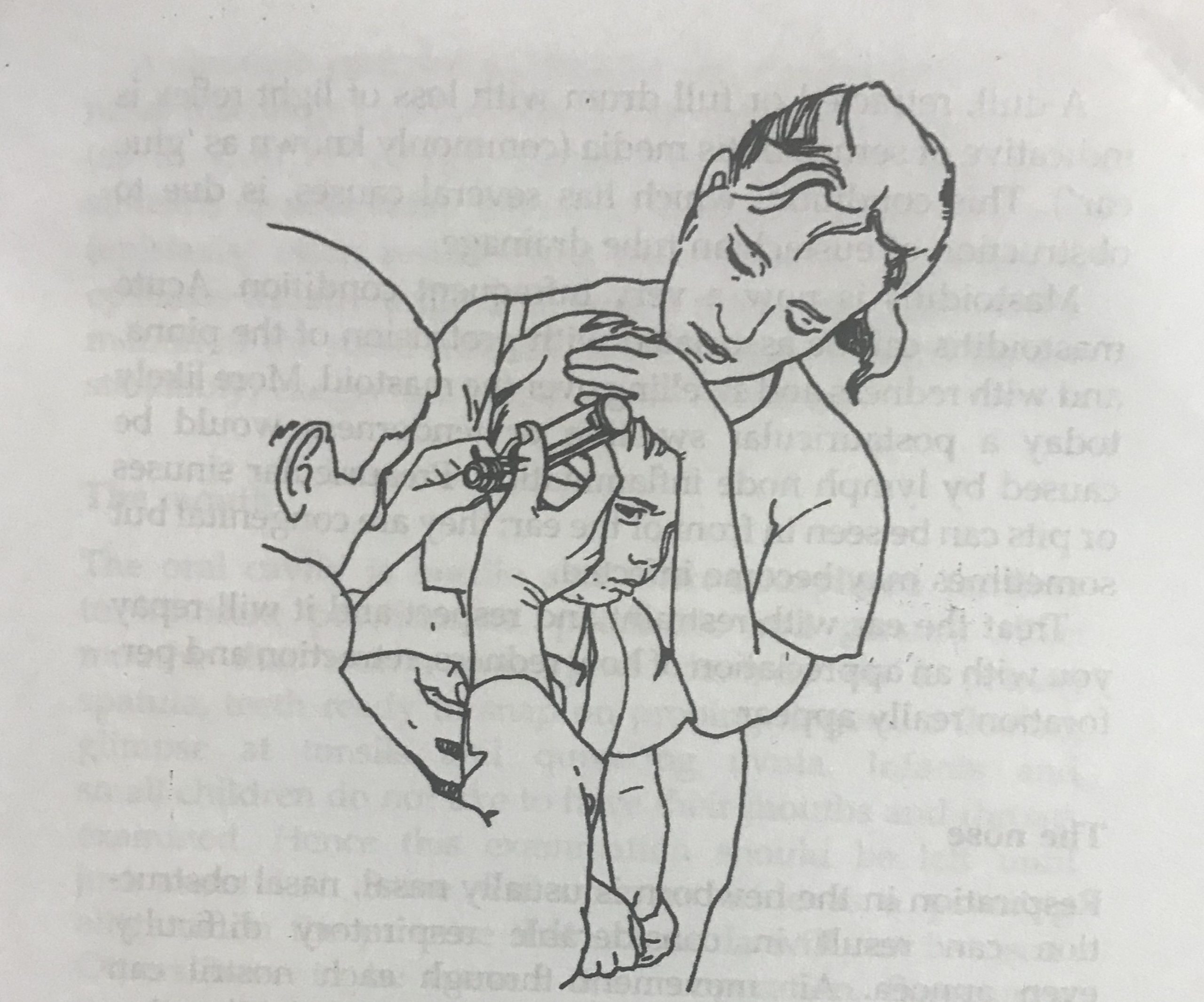
Photo (13) holding a child for otoscopic examination
Seven ages of children
Children change, grow, mature and develop. One’s style and approach to physical examination will very much depend on the child’s age, independence and understanding. The seven ages of children are:
- Newborn, neonate = first month of life
- Infant = 1 month to 1 year
- Toddler = 1 year to 3 year
- Preschool child = 3 – 5 year
- School child = 5 – 18 year
- Child = 0 -18 year
- Adolescent = early: 10 -14 year
= late: 15-18 year
Growth, Development and Measurements
As a child is growing and developing, history and examination of growth and development is essential in pediatric examination. Also the measurement of anthropometric measures such as weight, height and occipito-frontal circumstances are necessary. These measurements should be plotted on the appropriate centile charts and documented for further comparison. Although it may not be possible in a busy general practitioner’s clinic, at least some basic anthropometric measures should be documented. More detailed growth and development examination may need to be done in a separate appointment with specially trained persons, for example in a Well Baby Clinic.
Tips for newborn examination
Most practitioners including pediatricians find neonatal examination to be difficult and challenging. It is true that the clinical features in these tiny babies are very non-specific and difficult to localize. One basic information is to know the features of a good newborn baby. These features include – looks pink ( tongue, oral mucosa), feels warm (felt over the covered area) , sucks well (can test with your clean or gloved little finger), strong cry and good tone (stretch a leg and release it ). The absence of one or more of these features indicate a serious problem in a newborn and should be referred to a pediatrician.
Tolerate and use the cry
Children can cry very frequently especially when they are ill. The cry is the language of children and a practitioner should not be disturbed by it. In general, we should accept that “If a child cries in your clinic, it is your fault and not a child’s. Instead of annoyance or disappointment the practitioner should tolerate and use a child’s cry for diagnosis. The infant’s ability to express himself is very limited, especially in his early days and months. His cry may be trying to tell you something. Mothers can recognize their baby’s different types of cry; so take it seriously if she says her baby’s cry has changed.
a. painful cry – high-pitched, shrill, screeching, screaming or piercing – meningitis, encephalitis, increased intracranial pressure
b. hoarse cry – croup
c. intussusception – sudden and grunting, recurring every few minutes and looks normal in-between. Loud screaming attacks which recurs at frequent intervals accompanied by straining efforts with leg and knee flexed
d. seriously ill infant – weak and whimpering
e. hoarse, croaky cry – congenital hypothyrioidism
f. infantile beriberi – weak but continuous grunting
“Veterinary” Pediatrics
By using the term “veterinary” we are not attempting to be comparing children to animals, but are trying to draw your attention to certain analogies between young children and animals. Some attributes shared by children and animals are :
- They don’t like being stared at
- They lie down when sick
- Repeated food refusal is unusual
- They have limited ability to express themselves
- They adopt the position of comfort when well
- Their survival instinct is strong
(photo 14 )
Photo (14) Veterinary Pediatrics
Conclusions
Most general practitioners will have to see children in their clinics, whether they like it or not. If you know the some useful tips of pediatric clinical examination, your clinical encounter with children can be much more enjoyable and successful.
Bibilography
- Gill N and O’Brien N. Paediatric Clinical Examination Made Easy. Churchill Livingstone, Elsevier. Edinburgh.2007.Fifth Edition.
- Liang I. A and McIntosh N. Paediatric history and clinical Examination. London.1994.
- Macleod J. Clinical Examination. Churchill Livingstone. Edinburgh and London. Third Edition, 1973: 372-411.
- Kliegman R. M, Blum N.J, Shah S.S, St Geme III J.W, Tasker R,C, Wilson K.M, Behrman R.E. Nelson Textbook of Pediatrics. ELSEVIER (Philadelphia). Twenty First Edition, 2020: 1965-1967 , 867-868
Author information
Saw Win
Consultant Pediatrician, Parami General Hospital
Former Professor / Head, Department of Paediatrics, UM 1 Yangon
MBBS, DCH, MMedSc( Paed.),MRCPCH, FRCPE,
DCH (Glas.), DTM&H( Lond.) Dip Med Ed,