
Introduction
Immunization has been globally accepted as the most effective way of saving lives. However, vaccine hesitancy becomes an alarming health problem around the globe which has been mentioned as one of the top ten treats to global health(1). Vaccination is an indispensible health measure and consequently, vaccine hesitancy is a major health hazard needed to be addressed and tackled as a top priority.
Definition
According to WHO,vaccine hesitancy refers to delay in acceptance or refusal of vaccines despite availability of vaccination services. Vaccine hesitancy is complex and context specific varying across time, place and vaccines (2). It includes factors such as complacency, convenience and confidence.
Spectrum of Vaccine Hesitancy
The hesitancy continuum extends from those that accept all vaccines, but are unsure about their decisions for some or all vaccines, through to those who refuse all vaccines, but are unsure about these decisions.Vaccine hesitant individuals belong to the middle of a spectrum of those who actively demand vaccine and those who completely refuse all vaccines. Simply put, hesitant individuals can refuse some vaccines but accept others; they may accept a vaccination and even do so according to schedule, but are unsure in the process or they may simply delay in accepting vaccines (3). Vaccine hesitancy could also exist in situations where vaccines are either unavailable or services are limited because of systems failures (e.g. stockouts, lack of vaccination services), natural or man-made disasters(3).
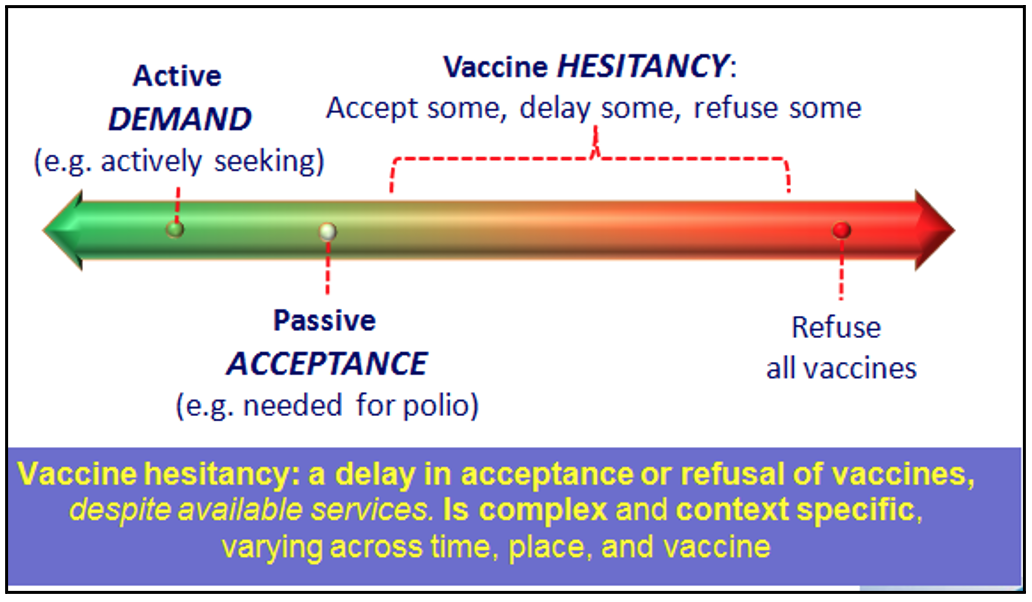
Figure (1) Spectrum of vaccine hesitancy (4)
Historical perspective of Vaccine Hesitancy
Vaccine hesitancy is actually not an emerging problem. Public questioning of vaccine is as old as vaccine itself. Vaccine refusal has always been associated with many outbreaks in many countries through the ages (5). From the very early history of vaccination, really from the first time Edward Jenner developed an effective vaccine against smallpox in 1796,there were groups of people who were nervous, hesitant or resistant to vaccination due to religious or safety concern (6). There has been a lot of objection when vaccination has been made compulsory in particular.In modern history of anti-vaccination, there were notable events like the 1982 broadcast of DPT: Vaccine Roulette, which sparked debate over the DPT vaccine, (7) and the 1998 publication of a fraudulent academic article by Andrew Wakefield (6) which sparked the MMR vaccine controversy. Also recently, the HPV vaccine has become controversial due to concerns that it may encourage promiscuity when given to 11- and 12-year-old girls (8). It has been assumed that arguments against vaccines in the 21st century are often similar to those of 19th-century anti-vaccinationists (7).
Prevalence of Vaccine Hesitancy
Vaccine currently saves two to three millions deaths a year but further 1.5 million could be avoided if global coverage of vaccine improved. Measles cases have been increased by30 % worldwide due to vaccine hesitancy (9). According to WHO data, hesitancy is present in the majority of countries globally with less than 10% reporting no hesitancy (10)
In a global survey regarding vaccine confidence,althoughoverall vaccine confidence is positive, responses differ between countries.The European region has the lowest confidence in vaccine safety with France the least confident globally.Bangladesh, Ecuador, and Iran reported highest agreement that vaccines are important while Azerbaijan, Russia, and Italy reported most skepticism around vaccine importance. Notably, education increases confidence in vaccine importance and effectiveness but not safety (11).
Current situation in Myanmar
Previously in Myanmar, reasons for missed opportunities of immunization are mostly poor socioeconomic status, geographic reason, and security concern in ethnic groups. Recently, social media become popular in Myanmar, making easier to create, consume, and share unverified, anecdotal information posing as facts.Consequently, anti-vaccine movement has proliferated, using social media to churn out often misleading information in recently. Many Myanmar doctors, social influencers and authority have confronted with great effort to eliminate anti vaxxer fear on social media.
Major contributing factors of Vaccine Hesitancy
To address the vaccine hesitancy within a country and/or subgroup, it is required to understand the magnitude and setting of the problem, diagnosis of the root causes, tailored evidence-based strategies to address the causes, monitoring and evaluation to determine the impact of the intervention and whethervaccine acceptance has improved, and ongoing monitoring for possible recurrence of the problem (2).
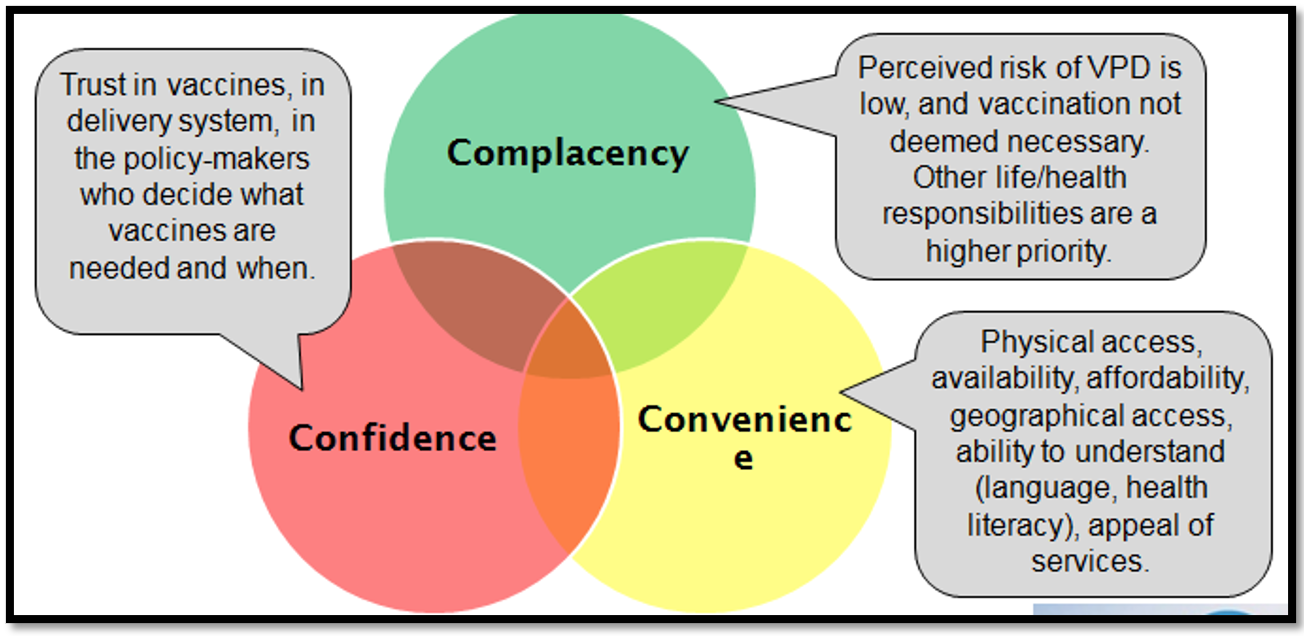
Figure (2) Major contributing factors of vaccine hesitancy (12)
The WHO EURO Vaccine Communications Working Group has proposed a model to explore the causes of vaccine hesitancy known as the “3C’s”: complacency, convenience and confidence (12).In the “3 Cs” model, confidence is defined as trust in (i) the effectiveness and safety of vaccines; (ii) the system that delivers them, including the reliability and competence of the health services and health professionals and (iii) the motivations of policy-makers who decide on the needed vaccines(3).
Vaccination complacency exists where perceived risks of vaccine-preventable diseases are low and vaccination is not deemed a necessary preventive action. Complacency about a particular vaccine or about vaccination in general is influenced by many factors, including other life/health responsibilities that may be seen to be more important at that point in time. Immunization programme success may, paradoxically, result in complacency and ultimately, hesitancy, as individuals weigh risks of vaccination with a particular vaccine against risks of the disease the vaccine prevents that disease is no longer common. Self-efficacy (the self-perceived or real ability of an individual to take action to be vaccinated) also influences the degree to which complacency determines hesitancy (3).
Vaccination convenience is a significant factor when physical availability, affordability and willingness-to-pay, geographical accessibility, ability to understand (language and health literacy) and appeal of immunization services affect uptake. The quality of the service (real and/or perceived) and the degree to which vaccination services are delivered at a time and place and in a cultural context that is convenient and comfortable also affect the decision to be vaccinated and could lead to vaccine hesitancy(3).
Reasons for vaccine hesitancy
To tackle the problem of vaccine hesitancy, detailed research to understand the reasons for vaccine hesitancy is an important step. According to the GVAP Secretariat Report 2016, the major reasons for vaccine hesitancy are as follows:
(a) Risk-benefit issues of the vaccine, particularly concerns about safety
(b)Knowledge / awareness issues around vaccines
(c) Religion, culture, gender, and socioeconomic issues
(d)Design of programme / Mode of delivery. (13)
Strategy to overcome vaccine hesitancy
In 2014, a systematic review of strategies peer-reviewed and grey literature (2007-2013) and a review of reviews identified that vaccine hesitancy is a complex problem andmulti-component approach is more effective than single component approach to sort it out this complicated issue. There are 8 core approaches to handle the vaccine hesitancy(14):
“Preventive” routine activities:
1. Strengthen programme coordination
2. Build stakeholder relations
3. Improve communications and information
4. Boost health worker practice
Tailored “responses”:
5. Diagnose vulnerable populations
6. Do not dismiss refusers or the hesitant
7. Tailor discussion techniques
8. Address concerns about safety, pain, and multiple injections
1. Strengthen programme coordination
It is necessary to establish mechanisms for regular coordination and information-sharing (e.g. communications working group):
- Plan and budget for activities in advance
- Ensure buy-in and approval at all appropriate levels, including the Minister
- Promote evidence-based national policy-making (e.g. NITAG)
- Identify and spokespeople, and align on messaging
Planning for an emerging event is important: pre-agreed processes, roles, and responsibilitiestofacilitate a rapid and well-coordinated response when needed(14).
2. Build stakeholder relations
Building stakeholder relations is an important strategy in dealing with vaccine hesitancy since collaboration between national authorities, academia and experts , professional associations, non-governmental organization, civil society , private sector , global agencies and media is needed to share information and coordination , to empower key voices , to amplify consistent messaging to enhance health worker credibility to save time and resources and maintain a positive and supportive environment to achieve ultimate outcome of tackling vaccine hesitancy(15).
3. Improve communications and information
Building an awareness of vaccine safety and disease susceptibility is essential strategy which can be achieved by listening and monitoring to understand the causes of hesitancy, tailoring and test evidence-informed interventions, contextualising for content, design, and format and evaluating process and impact, and adjusting as needed (15 ). Moreover, the media plays a significant role in propagating vaccine hesitancy, especially in spreading controversial stories. It is therefore recommended that health information should be proactive, focused on the needs of the population and apply a variety of social media platforms. Enough information on the rigour of vaccine development has been suggested to improve acceptance of vaccination (3).
4. Boost health worker practice
Boosting the practice of health worker in vaccination is an obligatory strategy. Supporting health workers with regular and quality training and tools, ensuring availability of accurate information on disease risks, vaccine safety and benefits are good practices. Complement training with regular supportive supervision to reinforce skills and guide corrective action is also a pivotal action in improving vaccine acceptance(15).
5. Diagnose vulnerable populations
It is stated that reasons for hesitancy vary in each population. To achieve high and equitable vaccination uptake, it is necessary to understand the barriers to vaccination for the specific population groups(14). Then solutions can be designed which support, motivate and enable people to be vaccinated, regardless of who or where they are
The “Tailoring Immunization Programmes” approach can help national programmes to: identify susceptible population groups (16).
6. Do not dismiss refusers or the hesitant
Many factors determine vaccination beliefs and behaviours and those attitudes would not be changed easily. Hence, building trust via caring andcompetence an understanding the public concerns is mandatory to tailor responses to the concerns expressed (make no assumptions) (14).
9. Tailor discussion techniques
To achieve the ultimate goal of reducing vaccine hesitancy, individualized discussion techniques should be used to fit the individual concern. Client-centred, goal oriented discussion is necessary to change behaviour by strengthening personal motivation. Moreover, an atmosphere of acceptance and compassion should be offered (17).
Conclusion
Vaccine Hesitancy is one of the ten threats to global health. Although it is not a major problem at present in Myanmar with the increasing utilization of social media it can become an important problem. Vaccine preventable diseases remains a major health issues in Myanmar and progress in control of these diseases can be seriously affected by vaccine hesitancy. All medical professionals in Myanmar need to prepare themselves on how to effectively deal with this potential problem.
References
- World Health Organisation. 2019.Ten threats to global health in 2019 Available from: <https://www.who.int/emergencies/ten-threats-to-global-health-in-2019> . [Accessed date 10 November 2019].
- World Health Organization (WHO), Strategic Advisory Group of Experts on Immunization (SAGE). 2015 Summary WHO SAGE conclusions and recommendations on Vaccine Hesitancy, Geneva: WHO, 2015
- Swedish network for international health , Is vaccination a victim of its own success? 2019. Available from <https://www.snih.org/calvin-is-vaccination-a-victim-of-its-own-success/>. [Accessed date 10 November 2019].
- World Health Organization (WHO), Strategic Advisory Group of Experts on Vaccine Hesitancy, Final Report. October 2014. Geneva: WHO, 2014.
- Dubé E, Vivion M, MacDonald NE. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact, and implications. Expert Rev Vaccines. 2015; 14(1):99-117
- “Communicating science-based messages on vaccines”. Bulletin of the World Health Organization. 95 (10): 670–71. October 2017.. Geneva: WHO, 2017.
- Wolfe RM, Sharp LK. Anti-vaccinationists past and present. BMJ. 2002; 325 (7361): 430-2
- Knox R. HPV Vaccine: The Science Behind The Controversy .Available from <https://www.npr.org/2011/09/19/140543977/hpv-vaccine-the-science-behind-the-controversy>[Accessed date 10 November 2019].
- World Health Organization. 2018. Measles cases spike globally due to gaps in vaccination coverage Available from:<https://www.who.int/emergencies/ten-threats-to-global-health-in-2019> .[Accessed date 10 November 2019]
- World Health Organization (WHO), United Nations Children’s Fund (UNICEF)
Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting Form data-2015–2017 ,Geneva: WHO, 2018. - Heidi J.Larson, WilliamS.Schulz,PierreVerger, IainNickS.Jones:2016. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey . Available from < https://doi.org/10.1016/j.ebiom.2016.08.042>. [Accessed date 10 November 2019].
- Noni E. MacDonald. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015 Aug:4161-4
- World Health Organization. (2016) GVAP Secretariat Report 2016. Available from: <http://www.who.int/immunization/global_vaccine_action_plan/gvap_secretariat_report_2016.pdf > . [Accessed date 10 November 2019].
- Dube E, Gagnon D, MacDonald NE .Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine. 2015;33(34):4191-203
- Thomson A, Watson M. (2016) Vaccine hesitancy: a vade mecum v1.0. Vaccine. 34;2016.
- World Health Organization. (2018) Tailoring Immunization Programme .Available from: <https://www.who.int/immunization/programmes_systems/ Global_TIP_overview_July2018.pdf?ua=1> .[Accessed date 10 November 2019].
- Opel, D., Heritage , J., Taylor,J., Mangione-Smith,R., Salas, H., DeVere, Chuan Zhou, and Robinson.D.The Architecture of Provider-Parent Vaccine Discussions at Health Supervision Visits Pediatrics. 2013 Dec; 132(6): 1037–1046.
Saw Win@, Kyi San Thi
MBBS,DCH ,M Medsc (Paed.), MRCPCH, FRCP,DCH(Glas.), DTM&H(Lond.), Dip Med Edu, Senior Consultant Paediatrician, Parami General Hospital, Member WHO-SEAR-ITAG
# MBBS, M MedSc (Paed.), MRCPCH – Assistant Lecturer, Department of Pediatrics, University of Medicine 2, Yangon
