Dr. Kyaw Htay Lwin, M.B.B.,S M.Med.Sc (Surgery), MRCSEd, Consultant Surgeon, PHSH
Abstract: 39- year- Caucasian, vegetarian lady with fecal loaded redundant sigmoid colon was a probable cause of a sigmoid volvulus.
Introduction: A volvulus or torsion of a segment of the alimentary tract often leads to bowel obstruction needing surgical intervention. The most common sites are the Sigmoid colon and Caecum.
Sigmoid Volvulus is a condition in which the sigmoid colon wraps around itself and its own mesentery causing closed-loop obstruction. It represents 4% of all cases of large bowel obstruction in developed countries and 50% in developing countries. It usually affects adults, with the highest incidence seen in the 4th– 8th decades of life. More common in male and occur in ratio ranging from 2:1 to 10:1 compared to female. Predisposing anatomical features such as a redundant sigmoid colon with a narrow mesenteric attachment and fecal loaded colon should be the probable causes although the precise pathogenesis has not yet been well established. Patients usually present with triad of abdominal pain, constipation and abdominal distention. There may also be vomiting, empty rectal ampulla, and associated mental and other medical illness.
Case presentation
39-year-old Caucasian (tourist) lady, a vegetarian presented to emergency department with the severe generalized abdominal pain (pain score of 10/10) with marked abdominal distention. She had suffered from sub-acute intermittent abdominal discomfort for approximately 2 weeks during her tour trip to Bagan. There was also absence of stool for about one week and no flatus for 4~5 days. History ruled out no relevant medical problem apart from habitual constipation which needs regular laxatives.
Upon clinical examination, body temperature of 37.5 celsius, blood pressure of 130/90 mmhg and pulse rate of 110 per minute. There was a diffuse abdominal tenderness and gaseous distention without guarding and rebound tenderness. Slight reduced in bowel sound and empty rectum in rectal examination.
Blood analysis revealed slight increased in C – reactive protein and white cell counts of 12.72.
Supine and erect plain abdominal films showed signs of fecal impaction in the ascending and part of transverse colons, gas filled distended left colon and a distended sigmoid loop filled with fecolith showed inverted U configuration (Omega loop sign and coffee bean sign). Subsequent CT scan abdomen also showed fecal loaded sigmoid segment suggestive of sigmoid volvulus.
After the necessary replacements and measures, emergency laparotomy was performed 3 –hours after arrival to the hospital.
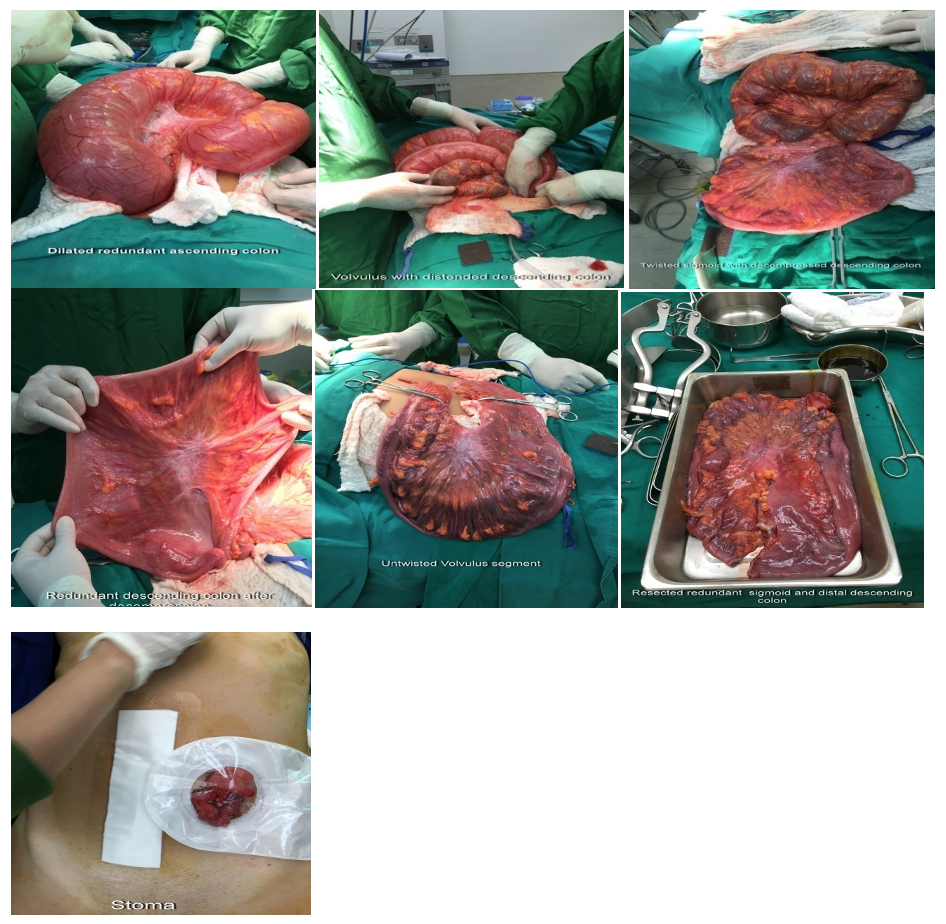
Laparotomy uncovered the volvulus of sigmoid colon at the colo-sigmoid junction, distended helices (diameter of ~11 cm) filled with stool and marked gaseous dilatation of transverse and descending colons and fecal loaded dilated ascending colon.
Fecal loaded sigmoid segment was twisted ~ 270 (counter-clock wise) degrees and found to be barely viable. Apart from that, the rest of the colon was grossly viable.
After proper decompression of the colon was performed proximal to the site of obstruction, untwisted sigmoid segment was resected along with the redundant portion including part of distal descending colon (about 18 inches length).
Since there was a marked discrepancy of the diameters of the ends of the resected colon, double barrel stoma was created instead of primary end to end anastomosis. Anatomo-pathological examination of the specimen confirmed ischaemic thin wall and transmural active inflammation. Histopathological examination showed no malignancy and evidence of tuberculosis.
Post-operative period was uneventful and she was discharged on 5th – post-operative day with stoma.
Further plan is to fly back to Singapore and stoma closure will be done at a later days.
Discussion
The sigmoid volvulus obstruction has been diagnosed based on clinical, imaging results and surgical exploration revealed the final diagnosed in this lady. The correct timing of the surgery prevents the risk of perforation of sigmoid colon and subsequent fatal fecal peritonitis.
The weight of the fecal loaded redundant sigmoid probably caused the rotation around its mesocolon and thus causing a real sigmoid volvulus. The habitual constipation and high fiber diet may probably be the other contributing factors.
Decompression through colonoscopy was not attempted because of the days of pain history. This kind of history is considered to be an absolute contraindication for decompression through colonoscopy because of the risk of existing ischemic colon necrosis, which could lead to bowel perforation during the colonoscopic distortion attempt.
Although some conservative measures can be applied to ameliorate the symptoms caused by volvulus, surgical exploration and resection is the most definitive approach in this particular patient since fecal impaction of redundant sigmoid is the probable cause of obstruction.
Conclusion
This case described relatively young age (ie: 39) lady presented with history of habitual constipation and symptoms of large bowel obstruction which was diagnosed as sigmoid volvulus secondary to fecal impaction of the large redundant sigmoid colon.
Surgical exploration, resection of the ischaemic volvulus segment and the redundant portions of colon not only relieved the obstruction but also prevent the recurrent attack.
Choice of treatment modalities and correct timing of the surgery is very important in order to avoid fatal complications of the Sigmoid Volvulus.
References
- BAKER D. M., WARDROP P. J., BURRELL H. et al. The management of acute sigmoid volvulus in Nottingham. J R CollSurgEdinb, 1994, 39 : 304.
- Lal SK, Morgenstern R, Vinjirayer EP, Matin A. Sigmoid volvulus an update. GastrointestEndoscClin N Am. 2006;16:175–187. [PubMed] [Google Scholar]
- Kuzu MA, Aslar AK, Soran A, Polat A, Topcu O, Hengirmen S. Emergent resection for acute sigmoid volvulus: results of 106 consecutive cases. Dis Colon Rectum. 2002;45:1085–1090. [PubMed] [Google Scholar]
- Chung YF, Eu KW, Nyam DC, Leong AF, Ho YH, Seow-Choen F. Minimizing recurrence after sigmoid volvulus. Br J Surg. 1999;86:231–233. [PubMed] [Google Scholar]
- Oren D, Atamanalp SS, Aydinli B, Yildirgan MI, Basoglu M, Polat KY, Onbas O. An algorithm for the management of sigmoid colon volvulus and the safety of primary resection: experience with 827 cases. Dis Colon Rectum. 2007;50:489–497. [PubMed] [Google Scholar]
- Akcan A, Akyildiz H, Artis T, Yilmaz N, Sozuer E. Feasibility of single-stage resection and primary anastomosis in patients with acute noncomplicated sigmoid volvulus. Am J Surg. 2007;193:421–426. [PubMed] [Google Scholar]