Incidence and Epidemiology
Benign Prostatic Hyperplasia (BPH) is the most common benign tumour in men and its incidence is age-related. The prevalence of histologic evidence of BPH in autopsy is 50% in men aged 51–60, and rises gradually up to 90% in men older than 80 years. Symptoms of prostatic obstruction are also age-related. At age 55, approximately 25% of men report obstructive voiding symptoms. However, it must be noted that the degree of bladder outlet obstruction is not directly related to size of the prostate.
Aetiology
The aetiology of BPH is poorly understood but it seems to be multifactorial and endocrine-controlled. Investigations have demonstrated a positive correlation between levels of free testosterone and oestrogen and the volume of BPH. The latter may suggest that the association between aging and BPH might result from the increased oestrogen levels of aging causing induction of the androgen receptor, which thereby sensitizes the prostate to free testosterone. There is evidence that oestrogens acting through stromal and epithelial oestrogen receptors may contribute to hyperplasia of the prostate.
Pathology
BPH develops in the transition zone and periurethral glands (See Fig:1). It is truly a hyperplastic process resulting from an increase in cell number. Microscopic evaluation reveals a nodular growth pattern that is composed of varying amounts of stroma and epithelium. Stroma is composed of varying amounts of collagen and smooth muscle. The differential representation of the histologic components of BPH explains, in part, the potential responsiveness to medical therapy. Thus, α-blocker therapy may result in excellent responses in patients with BPH that has a significant component of smooth muscle, while those with BPH predominantly composed of epithelium might respond better to 5α-reductase inhibitors. Patients with significant components of collagen in the stroma may not respond to either form of medical therapy. Please remember this fact in choosing the type of medication in different types of BPH on Digital Rectal Examination (DRE) findings and ultrasound findings.
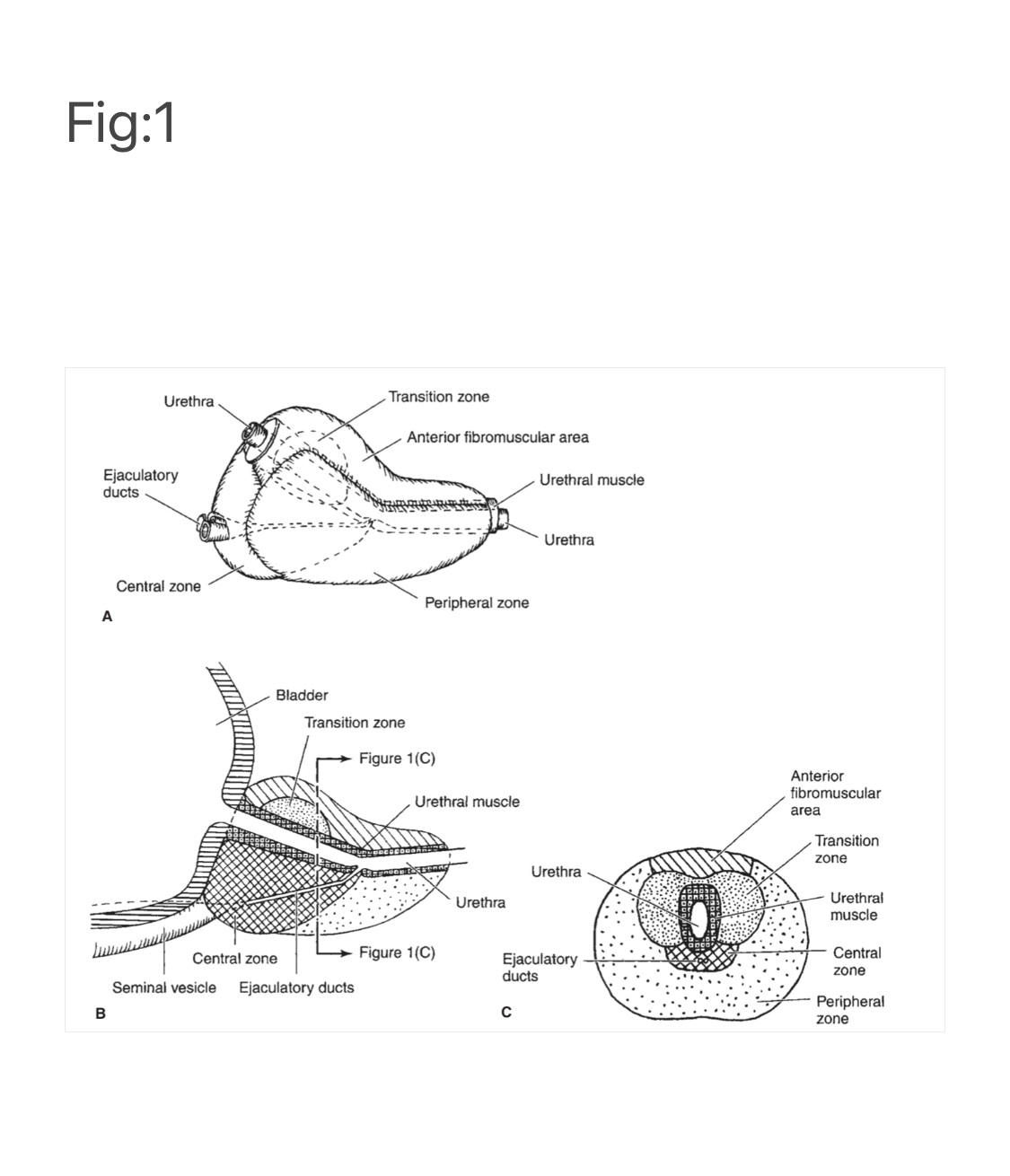
Fig 1
Pathophysiology
The pathophysiology of BPH is complex. Prostatic hyperplasia increases urethral resistance, resulting in compensatory changes in bladder function. However, the elevated detrusor pressure required to maintain urinary flow in the presence of increased outflow resistance occurs at the expense of normal bladder storage function. Obstruction-induced changes in detrusor function, compounded by age-related changes in both bladder and nervous system function, lead to urinary frequency, urgency, and nocturia, the most bothersome BPH-related complaints. Thus an understanding of BPH pathophysiology requires detailed insight into obstruction-induced bladder dysfunction.
Clinical Findings
Symptoms
The symptoms of BPH can be divided into “irritative” and “obstructive”. Combination of these symptoms is called Lower Urinary Tract Symptoms (LUTS), which is the term commonly used now-a-days.
Irritative symptoms include urgency, frequency, and nocturia. Irritative symptoms tend to appear earlier.
Obstructive symptoms are hesitancy, decreased force and caliber of stream, sensation of incomplete bladder emptying, double voiding (urinating a second time within 2 hours of the previous void), straining to urinate, and postvoid dribbling.
The symptoms are best assessed by IPSS. However, due to the variable acceptance and understanding of the patients, often the evaluation results are not quite satisfactory.
International Prostate Symptom Score (IPSS) (Table 1)
This assessment focuses on seven items that ask patients to quantify the severity of their obstructive or irritative complaints on a scale of 0–5. Thus, the score can range from 0 to 35. An IPSS of 0–7 is considered mild, 8–19 is considered moderate, and 20–35 is considered severe.
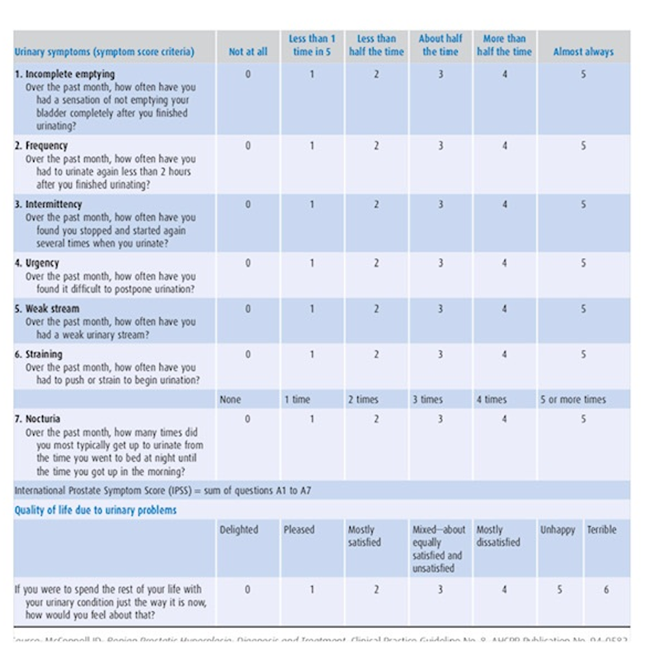
Table 1 International Prostate Symptom Score (IPSS)
A detailed history focusing on the urinary tract may exclude other possible causes of symptoms that may not result from the prostate, such as urinary tract infection, neurogenic bladder, urethral stricture, or prostate cancer.
Signs
A general physical examination, Digital Rectal Examination (DRE) and focused neurologic examination need to beperformed on all patients. The size and consistency of the prostate are noted, even though prostate size, as determined by DRE, does not correlate well with severity of symptoms or degree of obstruction. BPH usually results in a smooth, firm, elastic enlargement of the prostate. Induration, if detected, must alert the physician to the possibility of Cancer of the prostate (CaP) and the need for further evaluation such as Prostatic specific antigen [PSA], transrectal ultrasound [TRUS] and biopsy.Other suspicious signs on DRE include nodularity and asymmetrical enlargement of prostate lobes.
Laboratory Tests
A urinalysis to exclude infection or hematuria and serum creatinine measurement to assess renal function are required. Serum PSA (Total) should be done in all cases particularly in patients with suspicious signs on DRE as mentioned above. Interpretation of PSA is complex. It should be adjusted according to age, race, and presence of family history. Often, PSA (Free) needs to be done in suspicious case to check free and total PSA ratio.
Imaging
Transabdominal Ultrasound should be done in all cases. Computed tomography [CT] Urogram is recommended only in the presence of concomitant urinary tract disease or complications from BPH (e.g, hematuria, urinary tract infection, renal insufficiency, history of stone disease). Transrectal Ultrasound (TRUS) is advisable if malignancy is suspected on DRE.
Cystoscopy
Cystoscopy is not routinely recommended to determine the need for treatment but may assist in assessing the size of diverticulum if present. If BPH is associated with hematuria, then cystoscopy is mandatory to rule out other bladder pathology.
Additional Tests
Measurement of urine flow rate, determination of postvoid residual urine, and pressure-flow studies are considered optional. Cystometrograms and urodynamic studies are reserved for patients with suspected neurologic disease or those who have failed prostate surgery.
Differential Diagnosis
Other obstructive conditions of the lower urinary tract, such as urethral stricture, high bladder neck, bladder neck contracture, bladder stone, or CaP, must be entertained when evaluating men with presumptive BPH. A history of previous urethral instrumentation, urethritis, or trauma should be elucidated to exclude urethral stricture or bladder neck contracture. Hematuria and pain are commonly associated with bladder stones. CaP may be detected by abnormalities on the DRE or an elevated PSA.
A urinary tract infection, which can mimic the irritative symptoms of BPH, can be readily identified by urinalysis and culture; however, a urinary tract infection can also be a complication of BPH. Although irritative voiding complaints are also associated with carcinoma of the bladder, especially carcinoma in situ, the urinalysis usually shows evidence of hematuria. Likewise, patients with neurogenic bladder disorders may have many of the signs and symptoms of BPH, but a history of neurologic disease, like Parkinsonism, stroke, diabetes mellitus, or spine injury may be present as well. In addition, examination may show diminished perineal or lower extremity sensation or alterations in rectal sphincter tone or the bulbocavernosus reflex. Simultaneous alterations in bowel function (constipation) might also alert one to the possibility of a neurologic origin.
Treatment
After patients have been evaluated, they should be informed of the various therapeutic options for BPH. As previously mentioned, most of the elderly Myanmar patients cannot give the realistic information related to their actual problems. Therefore, medical treatment can be started in patients with mild to moderate symptoms.
Medical Therapy
I. Alpha Blockers
The human prostate and bladder neck contains αlpha 1-adrenoreceptors, and the prostate shows a contractile response to corresponding agonists. The contractile properties of the prostate and bladder neck seem to be mediated primarily by the subtype αlpha1a-receptors. Alpha-Blockade has been shown to result in both objective and subjective degrees of improvement in the obstructive and irritative symptoms and signs of BPH in some patients. Alpha-Blockers can be classified according to their receptor selectivity as well as their half-life.
Phenoxybenzamine and prazosin are the prototypical nonselective and selective α-blockers, but today, they are primarily of historical interest.
Long-acting α1-blockers make once-a-day dosing possible, but dose titration is still necessary.
- Terazosin is initiated at 1 mg daily for 3 days and increased to 2 mg to 5 mg daily provided the fall in the blood pressure is acceptable.
- Doxazosin is started at 1 mg daily for 7 days and increased to 2 mg daily. Dosage can be escalated to 4 mg daily if necessary. Possible side effects include orthostatic hypotension, dizziness, tiredness, retrograde ejaculation, rhinitis, and headache.
Selective blockade of the α1a-receptors, which are localized in the prostate and bladder neck, results in fewer systemic side effects.
The followings are Alpha1a-Selective blockers. - Tamsulosin
Dose: 0.4 or 0.8 mg daily - Alfuzosin
Dose:10 mg daily - Silodosin
Dose: 8 mg daily
The action of alpha blockers can be achieved within 5 to 7 days. Always remember that Alpha blockers tend to have cardiovascular side effects, thus obviating the need for dose titration with these agents. Other side effect includes retrograde ejaculation.4
II. 5α-Reductase inhibitors
5 Alpha Reductase inhibitors—Finasteride is a 5α-reductase inhibitor that blocks the conversion of testosterone to active form dihydrotestosterone (DHT). This drug affects the epithelial component of the prostate, resulting in a reduction in the size of the gland and improvement in symptoms. Six-month therapy is required to see the maximum effects on prostate size (20% reduction).
Side effects are uncommon and include decreased libido, decreased ejaculate volume, and impotence. Serum PSA is reduced by approximately 50% in patients being treated with finasteride, but individual values may vary.
Dutasteride differs from finasteride as it inhibits both isoenzymes of 5α-reductase. Similar to finasteride, it reduces serum PSA and total prostate volume. Randomized, placebo- controlled trials have shown the efficacy of dutasteride in symptomatic relief, symptoms scores, peak urinary flow rate, and reduced risk of acute urinary retention and the need for surgery. Side effects are relatively uncommon and include erectile dysfunction, decreased libido, gynecomastia, and ejaculation disorders.
- Finasteride , dose 5 mg daily
- Dutasterid,dose 0.5 mg daily
Dutastride has dual actions. Therefore, effectiveness can be achieved earlier, as earlier as three months. The minimum length of time to take these medicines are 2 years when the size of the prostate can be reduced up to 20 percent.5
III. Combination therapy
If there is no contraindication, we can start with alpha blockers once diagnosis is made. And see the response in 5 to 7 days. We can add 5 Alpha reductase inhibitors in large glandular prostate. Generally speaking, those with soft prostate with more glandular elements tend to respond better with 5 Alpha reductase inhibitors.
Leopar and group in 1966 performed first randomized, double-blind, placebo-controlled study investigating combination α-blocker and 5α-reductase inhibitor therapy. It was a four- arm Veterans Administration Cooperative Trial comparing placebo, finasteride alone, terazosin alone, and combination finasteride and terazosin. More than 1200 patients participated, and significant decreases in IPSS and increases in urinary flow rates were seen only in the arms containing terazosin. However, one must note that enlarged prostates were not an entry criterion; in fact, prostate size in this study was much smaller than that in previous controlled trials using finasteride (32 vs 52 cm3). McConnell and colleagues in 2003 conducted a long- term, double-blind trial involving 3047 men to compare the effects of placebo, doxazosin, finasteride, and combination therapy on measures of the clinical progression of BPH . The risk of overall clinical progression—defined as an increase above baseline of at least four points in the IPSS, acute urinary retention, urinary incontinence, renal insufficiency, or recurrent urinary tract infection was significantly reduced by doxazosin (39% risk reduction) and finasteride (34% risk reduction), as compared with placebo. The reduction in risk associated with combination therapy (66% risk reduction) was significantly greater than that associated with doxazosin or finasteride alone. Patients most likely to benefit from combination therapy are those in whom baseline risk of progression is very high, generally patients with larger glands and higher PSA values.3
IV.Combined a-Blocker Therapy and Anticholinergic Therapy
Theoretically anticholinergics impairs detrusor muscle function but Patients with BPH often have concomitant bothersome irritative voiding symptoms due to overactive bladder (OAB), and thus selective anticholinergics are used to reduce the troublesome symptoms of the latter.
Anticholonergic (Tolterodine) is fairly good for OAB but now effect of Mirabegron is better. The latter is contraindicated in severe uncontrolled hypertension.1
V. PDE-5 Inhibitors
PDE-5 is present in human prostate and bladder tissue.
This, coupled with the observation that erectile function declines in men with increasing severity of LUTS, prompted an initial evaluation of PDE-5 inhibitors as a treatment for LUTS. Currently, low dose of tadalafil 5 mg can be used in patients with LUTS due to BPH and some degree of Erectile Dysfunction.2
VI.Phytotherapy
Phytotherapy refers to the use of plants or plant extracts for medicinal purposes. The use of phytotherapy in BPH has been popular in Europe for years, and its use in the United States is growing as a result of patient- driven enthusiasm. Several plant extracts have been popularised, including the saw palmetto berry (Serenoarepens), the bark of Pygeumafricanum, the roots of Echinacea pur- purea and Hypoxisrooperi, pollen extract, and the leaves of the trembling poplar. S. repens has been the most well- studied agent, usually at 320 mg/day. Given the poor regulation of the nutritional supplement industry, actual tablet content may vary extremely from the dose noted on the product label (Feifer et al, 2002). A prospective, randomized clinical trial of saw palmetto showed no benefit beyond placebo for either IPSS improvement or urinary flow rate (Bent et al, 2006). An updated systematic review including this and other trials confirmed no improvement over placebo for this approach (Wilt et al, 2009).1
Surgical Treatments
Indications for surgery
Surgical intervention is indicated when there is
- Failed medical treatment
- Urinary retention refractory to Trial Removal of Catheter (TWOC) after episode of acute urinary retention
- Complications related to bladder outlet obstruction due to BPH such as recurrent urinary tract infection, recurrent gross hematuria, bladder or kidney stones, renal insufficiency due to hydronephrosis and bladder diverticula formation.
Various types of surgical interventions
It is essential to note that there are various forms of treatments: invasive and minimally invasive. Choice of different modalities depend on the case scenario, availability of facilities, expertise and preference of the individual patient. Some forms of minimally invasive treatments do not stand the test of time and thus are not mentioned here at all or in details.6
Transurethral resection of the prostate (TURP)
It remains the gold standard treatment up to now taking into consideration of every factor although Laser Enucleation of prostate becomes popular in developed countries where cost is no longer a consideration. Most of these procedures involve the use of a spinal or general anesthesia and usually require short hospital stay.
Magnitude and durability of IPSS and flow rate improvement with transurethral resection of the prostate (TURP) is superior to that of any minimally invasive therapy. Risks of TURP include retrograde ejaculation (75%), impotence (5–10%), and incontinence (<1%).
Complications though less common include bleeding, urethral stricture or bladder neckcontracture; perforation of the prostate capsule with extravasations is very rare now-a-days.
TURP can now be performed with a bipolar electrode, allowing resection to be performed under saline irrigation. This approach eliminates the hyponatremia responsible for TUR syndrome, though significant fluid volume absorption can still occur with prolonged resection.
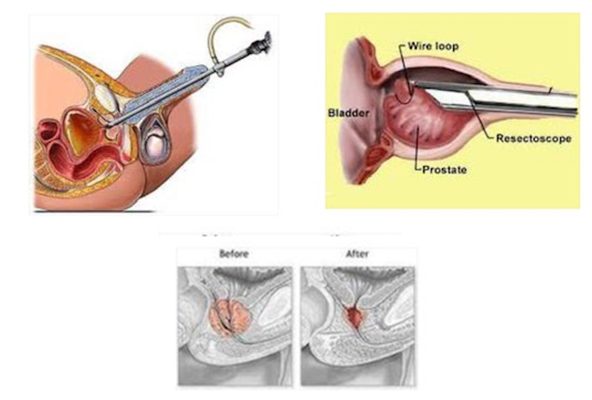
Fig 2: Transurethral Resection of Prostate
Transurethral incision of the prostate(TUIP)
Men with moderate to severe symptoms and a small prostate often have posterior commissure hyperplasia (elevated bladder neck). These patients will often benefit from an incision of the prostate. This procedure is more rapid and less morbid than TURP. Outcomes in well-selected patients are comparable, although a lower rate of retrograde ejaculation with trans- urethral incision has been reported (25%). The technique involves two incisions using the Collins knife at the 5- and 7-o’clock positions. The incisions are started just distal to the ureteral orifices and are extended outward to the verumontanum.
Transurethral vaporization of the prostate (TUVP)
These ablative techniques use photo- or electroevaporation to ablate obstructing prostate tissue. The two most commonly used devices for these procedures are the neodymium-doped yttrium-aluminum-garnet (Nd:YAG) KTP “Green Light” laser, which is preferentially absorbed by hemoglobin, and the plasma vaporization “Button” electrode. The latter works with a standard contemporary bipolar generator used for bipolar TURP.
As with modern TURP, these procedures are performed under saline irrigation. The goal of the procedure in either case is to produce a central prostate defect comparable with what would be expected after a traditional TURP, but withless bleeding and lower risk of perforation. The potential downsides are greater irritative voiding symptoms in the short term after the procedure and less durability of the result than a standard TURP. Also, as tissue is destroyed rather than resected, no specimen is sent to pathology for review. These techniques become less popular compared to the following HoLEP.
Holmium laser enucleation of the prostate (HoLEP)
Rather than progressive resection or ablation of tissue from the urethra outward as with TURP and its derivatives, HoLEP denotes an anatomic dissection in the plane between the central and peripheral zones of the prostate. This approach is felt to provide the largest defect and perhaps the longest durability, but entails a longer learning curve than TURP or TUVP.
The Holmium laser has a wavelength of 2,140 nm that is strongly absorbed by water.
The laser only penetrates 0.4 mm, resulting in precise tissue vaporization without deep coagulation or surrounding char effect.HoLEP involves trans-urethrally enucleating the individual lobes of the prostate with an end-firing Holmium laser and floating the enucleated lobes into the bladder. The prostate tissue is then removed with a transurethral mechanical morcellator.
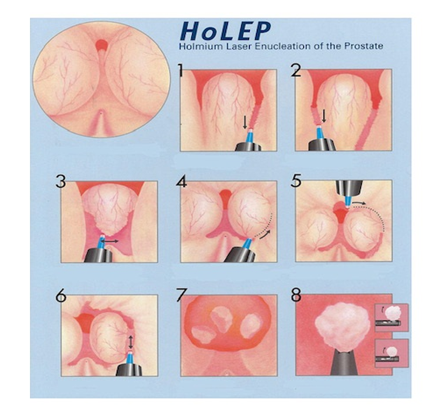
Fig 3: HoLEP
Transurethral enucleation of prostate with bipolar diathermy
Using the bipolar electrode with saline and double loops, enlarged obstructive prostate can be enucleated along the plane between the peripheral and transition zones and resected as shown in the figure.
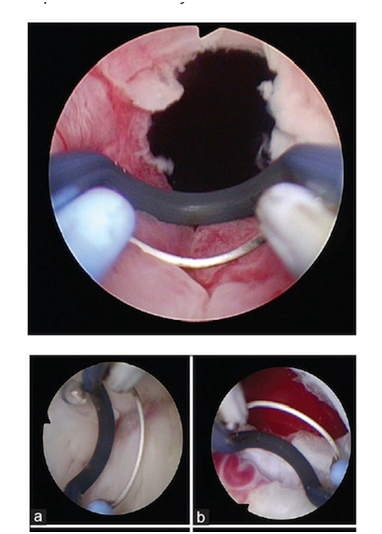
Fig 4: Transurethral enucleation with bipolar diathermy
Open prostatectomy
When the prostate is too large to be removed endoscopically, an open enucleation is necessary. What constitutes “too large” is subjective and will vary depending upon the surgeon’s experience with TURP. Glands >100 g are usually considered for open enucleation. Open prostatectomy may also be initiated when concomitant bladder diverticulum or a large bladder stone is present or if dorsal lithotomy positioning is not possible.
Open prostatectomies can be done with either a suprapubic or retropubic approach. A simple suprapubic prostatectomy is performed transvesically and is the operation of choice in dealing with concomitant bladder pathology. After the bladder is opened, a semicircular incision is made in the bladder mucosa, distal to the trigone. The dissection plane is initiated sharply, and then blunt dissection with the finger is performed to remove the adenoma. The apical dissection should be done sharply to avoid injury to the distal sphincteric mechanism. After the adenoma is removed, hemostasis is attained with suture ligatures, and both a urethral and a suprapubic catheter are inserted before closure. In a simple retropubic prostatectomy, the bladder is not entered. Rather, a transverse incision is made in the surgical capsule of the prostate, and the adenoma is enucleated as described earlier. Only a urethral catheter is needed at the end of the procedure. Robot-assisted simple prostatectomy has been reported in recent small series.
Conclusion
Benign Prostatic Hyperplasia is one of the commonest problems in urological practice. Since 5 decades ago, medical therapies have been much better and number of patients requiring surgical intervention is less with time. However, late diagnosis can lead to unnecessary consequences requiring surgery only at the very old age. The clinicians looking after a patient with LUTS need to exclude other causes like urethral meatal stenosis, phimosis, urethral stricture, neurogenic bladder and carcinoma of prostate. Digital Rectal Examination is a MUST in assessment and PSA (Total) should be done in all appropriate cases. PSA (Total) alone is not the diagnostic criteria for diagnosis for carcinoma. If suspicious, free PSA, Transrectal Ultrasound and biopsy needs to be done.
References
- Hutchison A, Farmer R, Verhamme K, et al. The efficacy of drugs for the treatment of LUTS/BPH, a study in 6 European countries. EurUrol 2007;51(1):207–15, discussion 215–206.
- Kohler T, McVary K. The relationship between erectile dysfunction and lower urinary tract symptoms and the role of phosphodiesterase type 5 inhibitors. EurUrol 2009;55(1):38–48.
- McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med 2003;349(25):2387–98.
- McNeill SA, Hargreave TB, Roehrborn CG. Alfuzosin 10 mg once daily in the management of acute urinary retention: results of a double-blind placebo-controlled study. Urology 2005;65(1):83–9, discussion 89–90.
- Roehrborn C, Siami P, Barkin J, et al. The effects of dutasteride, tamsulosin and combination therapy on lower urinary tract symptoms in men with benign prostatic hyperplasia and prostatic enlargement: 2-year results from the CombAT study. J Urol 2008;179(2):616–21, discussion 621.
- Wasson JH, Reda DJ, Bruskewitz RC, et al. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. The Veterans Affairs Cooperative Study Group on Transurethral Resection of the Prostate. N Engl J Med 1995;332(2):75–9.
Author Information
Toe Lwin
FRCS FACS DrMedSc
Former Professor & Head, Department of Urology
New Yangon General Hospital, University of Medicine1 Yangon