
Dr. Tin Zar Khine,
Dr. Khin Khin Mu,
Dr. Khin Saw Myint,
Dr. Myint Myint Sein,
Dr. Win Win Maw,
ABSTRACT
A total of one hundred clinically suspected otomycotic patients from Ear, Nose, Throat (ENT) OPD of North Okkalapa General and Teaching Hospital and Out Patient Department (OPD) of Ear, Nose and Throat Specialist Hospital, Yangon were included in this study. The ear swabs were collected from these patients and were examined for isolation and identification of fungal species at the mycology section, National Health Laboratory, during the period of January to September, 2014.
Out of 100 specimens, 83 specimens (83 %) yielded positive fungal culture. In 83 of the positive samples, 73 cultures had one kind of fungus and 10 cultures had mixed fungal growth.
The fungal pathogens isolated were Aspergillus species (63/83, 75.87%), Candida species (17/83, 20.44%), Cladosporium species (2/83, 2.40%) and Mucor species (1/83, 1.20%).
Single fungus was isolated from 87.87% (n=73) of fungal culture positive cases and two fungi were isolated from 12.05% (n=10) of cases. Aspergillus niger was the commonest (n=43, 51.80%), followed by Aspergillus flavus (n=11, 13.25%), other Aspergillus species (n=2, 2.40%), Aspergillus terreus (n=1, 1.20%), Aspergillus glaucus (n=1, 1.20%), Candida guilliermondii (n=6, 7.22%), Candida albicans (n=2, 2.40%), Candida parapsilosis (n=2, 2.40%) and Candida tropicalis (n=2, 2.40%). Of these 10 cases, six patients had coexisting Aspergillus niger and Candida guilliermondii, one patient had coexisting Aspergillus niger and Candida tropicalis, one patient had coexisting Aspergillus niger and Candida parapsilosis, one patient had coexisting Aspergillus niger and Candida albicans, one patient had coexisting Aspergillus glaucus and Candida tropicalis.
INTRODUCTION
Otomycosis is an acute, subacute or chronic fungal infection of the external auditory canal. It is a common fungal infection of the ear (Desai et al., 2012). It has been estimated that cases of otitis externa make up between 5 and 20% of otological consultations. Among them, only 15-20% are attributed to fungi (Gutierrez et al., 2005). Symptomatically, the condition may be indistinguishable from bacterial otitis externa although the irritation is usually more marked in fungal infections. Occasionally severe pain in the ear is the presenting symptom. On examination, a mass of greyish-white debris, resembling wet blotting paper, may be seen filling the meatus (Booth,1987 ).
The fungi that produce otomycosis are generally saprophytic fungi, Aspergillus niger, Aspergillus flavus, Aspergillus fumigatus, Penicillium species, Mucor, Rhizopus and Scopulariopsis. In addition, several yeasts, especially Candida species and dermatophytes (Epidermophyton floccosum, Trichophyton mentagrophytes and Trichophyton violaceum) cause otomycosis (Mogadam et al., 2009).
Aetiology of fungal pathogen and disease frequency vary according to different geographic zones, in relation to environmental factors (temperature, humidity) and the time of year. Treatment varies with different organism. Therefore, it is difficult to manage due to different factors related to the microorganism and the local and general characteristics of the patient. Although otomycosis is not a life threatening disease, recurrence is common and requires long term treatment.
To determine the fungal pathogens of otomycosis, a laboratory based cross-sectional descriptive study was done in 100 clinically diagnosed otomycotic patients seeking care at the Department of Ear, Nose and Throat, North Okkalarpa General and Teaching Hospital and Ear, Nose and Throat Hospital, Yangon and Mycology Section, National Health Laboratory, Yangon between January and October 2014.
MATERIALS AND METHODS
Collection and transport of specimens
After obtaining informed consent, clinical history was taken according to the proforma. The affected ear was examined first with an otoscope for confirmation of fungal infection. The fungal infection was seen as white or black debris. The fungal plug in the affected external ear was removed with the sterile cotton wool swab stick using an ear speculum. It was collected into the sterile test tube containing sterile normal saline.
Each specimen was labeled with the patient’s name, age, hospital registration number, date and time of collection. Then the samples were transported to the mycology section, National Health Laboratory, Yangon to be processed as soon as possible .
Isolation and identification of fungi
1. Microscopic examination of Potassium hydroxide wet mount under high power objectives and Gram – stained smearUsing oil immersion lens of an ordinary light microscope, the presence of bacteria, fungi, pus cells, and budding / non-budding yeast cells and hyphae were noted.5,7
2. Culture of the specimen
Under aseptic conditions, the specimen was inoculated into Sabouraud dextrose agar with chloramphenicol 0.05 mg / ml and Sabouraud dextrose agar with chloramphenicol 0.05 mg / ml and cyclohexamide 0.5 mg/ml to inhibit the growth of bacteria, fungal pathogens and saprophytic fungi. These inoculated tubes were incubated aerobically at 25ÿ C- 28ÿ C for up to 2 weeks.
3. Identification of species
3.1. Identification of species that formed
colonies resembling mold was done according to Forbes and Larone Method.
At every three days interval, culture tubes were examined for: rate of growth, texture (yeast-like, glabrous, powdery, granular, velvety or cottony), general topography (flat, heaped, regularly or irregularly folded), surface and reverse pigmentation and discarded after 2 weeks if there was no growth (Forbes et al., 2002; Larone, 2011).
(a) Aspergillus niger was identified by its rapid growth, maturation in 3 days, production of black surface with a white border; visibly composed of long, white to cream, erect hyphae with clusters of black conidia at the apices. Reverse surface showed white to cream color colonies.
(b) Aspergillus flavus showed rapid growth, maturation in 3 days and produced a yellow green to olive colour, often with specks of yellow; white border may be present. Texture was velvety to cottony. Reverse was usually yellowish to tan.
(c ) Aspergillus terreus was identified as cultures with colonies that are tan resemble cinnamon.
(d) Aspergillus glaucus showed moderately slow growth ( mature in 7-21 days ), surface felt like, dull green with yellow areas of cleistothecia production. Reverse surface of the culture was white to yellow.
(e) Cladosporium species has moderately rapid growth and maturation within 7 days at 25‡C. It produces greenish brown or black with grayish velvety nap, becoming heaped and slightly folded and reverse was black.
(f) Mucor species has rapid growth, mature within 4 days. It quickly covers agar surface with fluff resembling cotton candy; white in colour, later turns gray or grayish brown. Reverse was white.
Identification by Microscopic Examination of Growth
The definitive identification is based on the characteristic shape, method of production, and arrangement of spores and type and size of hyphae: the coenocytic (sparsely septate) hyphae of the Zygomycetes, the dark and pigmented septate hyphae of the dematiaceous fungi, and the septate, nonpigmented hyphae of the hyaline molds. The large, ribbon like hyphae of the Zygomycetes are easily recognized (Forbes et al., 2002).
Examination of lactophenol cotton blue mount (Tease mount)
A cover slip preparation with a drop of lactophenol cotton blue (LPCB) was examined under low (10x) and high power (40x) lens of the ordinary light microscope and the morphological features were carefully observed (Forbes et al., 2002; Larone, 2011).
MICROSCOPIC FINDINGS
Aspergillus species
Appearance of septate hyphae with long chains of brown to black, rough-walled conidia was identified as Aspergillus niger. Appearance of short chains of yellow-orange elliptical or spherical conidia was identified as Aspergillus flavus.
Aspergillus terreus was identified microscopically by appearance of vesicles which were hemispherical and phialides covers the entire surface and were produced from a primary row of branches. Phialides produced globose to elliptical conidia arranged in chains. Aspergillus glaucus produced septate hyphae and smooth conidiophores. The phialides are uniseriate and may be loosely columnar or radiate, covering most of vesicle and exhibiting round yellowish cleistothecia.
Cladosporium species
Micropically, the conidiophores are dark and branched with dark, septate hyphae, usually producing two or more conidial chains. Conidia are brown, round to oval and usually smooth, forming branching treelike chains and are easily dislodged, showing dark spots (hila) at the point where they were attached to the conidiophore or other conidia. The cells bearing the conidial chains are large, sometimes septate, resembling shields are called “shield cells”.
Mucor species
Microscopically, appearance of wide nonseptate hyphae were identified with long and branched Sporangiophores and bear terminal round, spore-filled sporangia. No rhizoids are formed.
Slide culture was also done on 1x1cm block of Sabouraud dextrose agar on a slide in a 100-mm diameter petri dish with a piece of wet filter paper and incubated at room temperature. The closed petri dish was placed on the microscope stage and the slide culture was examined with the low power (10x) objective. The examination was done periodically for growth and water was added if the plate began to dry out. The fungus grew on the surface of the slide and also on the undersurface of the cover slip. When reproductive structures were well developed, forceps were used to carefully remove the cover slip and placed it on a drop of lactophenol cotton blue on a second slide. The examination was done under the microscope with lowered light and at low or high power objective of ordinary light microscope.
Subculture on sporulating media(Potato dextrose agar)
Potato dextrose agar was used to stimulate the production of conidia and pigment and is recommended for inducing an isolate to exhibit a characteristic pigment (Larone, 2011).
B. Identification of fungal colonies resembling yeast
Identification of yeasts is based on cultural morphology, direct wet mount examination, Gram staining reaction and morphology, Germ tube formation test, Chlamydospore formation test, sugar fermentation test, and sugar assimilation test. These tests differentiate among yeasts based on their characteristic physiological reactions to various nutritional and environmental conditions and are similar to those used for bacteria. e (Howard et al., 1994; McGinnis, 1980; Larone, 1993; Odds, 1979).
RESULTS
Occurrence of otomycosis
Among 100 clinically suspected otomycosis patients, positive fungal culture was found in 83 patients (83%) and in (10.92%) of otitis externa.
The isolated frequency of fungus among clinically suspected cases was shown in Figure (1).
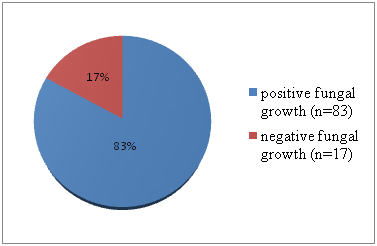
Figure 1. Isolated frequency of fungus from clinically suspected otomycotic patients
In 83 positive samples, 73 cultures had one kind of fungus and 10 cultures had mixed fungal growth.
The fungal pathogens isolated were Aspergillus species (63/83, 75.87%), Candida species (17/83, 20.44%), Cladosporium species (2/83, 2.40%) and Mucor species (1/83, 1.20%)[Plates: 5(A), 5(B), 6(A), 6(B), 6(C), 6(D), 6(E)]. Among them, Aspergillus niger was isolated from 43 patients (51.80%) followed by Aspergillus flavus from 11 patients (13.25%), other Aspergillus species from 2 patients (2.40%), Aspergillus terreus from 1 patients (1.20%) and Aspergillus glaucus from 1 patients (1.20%) [Plates: 1(A), 1(B), 1(C), 1(D), 2(A), 2(B), 2(C), 2(D), 3(A), 3(B), 3(C), 3(D), 3(E), 4 and 7].
Candida species isolated were Candida guilliermondii (n=6, 7.22%), Candida albicans (n=2, 2.40%), Candida parapsilosis (n=2, 2.40%) and Candida tropicalis (n=2, 2.40%) [Plates 8 and 9].
Table-1. Frequency of Aspergillus species and Candida species from otomycosis
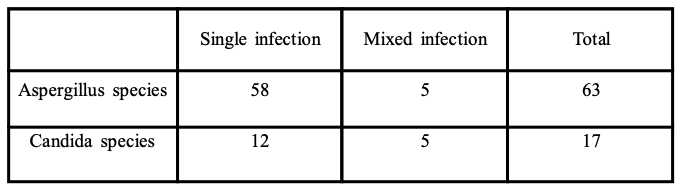

Plate 1(A). Aspergillus niger on Sabouraud dextrose agar slants
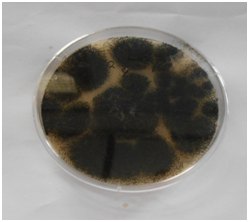
Plate 1(B). Aspergillus niger on Potato dextrose agar
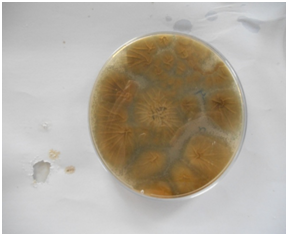
Plate 1(C). Aspergillus niger (Back view)
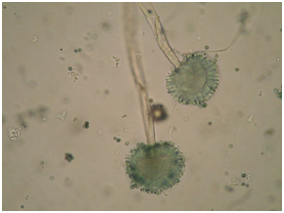
Plate 1(D). Microscopic appearance (lactophenol ) cotton Blue (400X, OLM)

Plate 2(A). Aspergillus flavus on Sabouraud dextrose agar slants
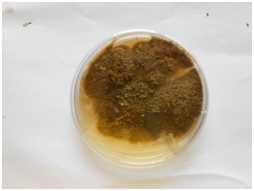
Plate 2(B). Potato dextrose agar plate

Plate 2(C). Back view of Aspergillus flavus
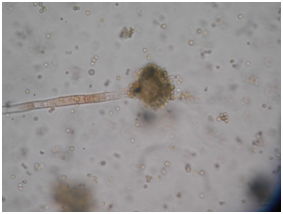
Plate 2(D). Microscopic appearance (Lactophenol cotton Blue (400X, OLM)
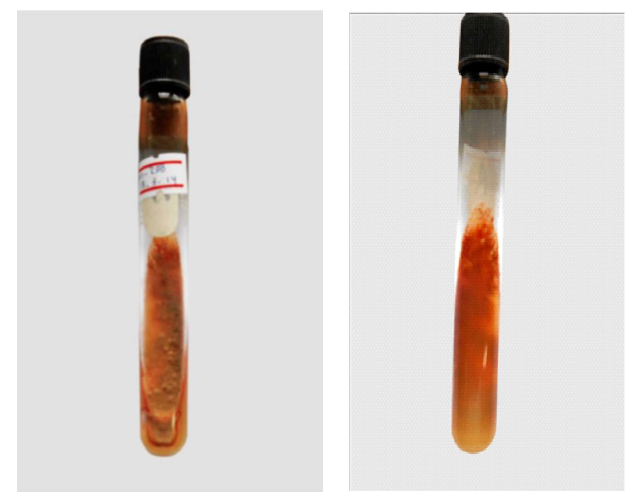
Plate 3(A) & (B) . Front and Back views of Aspergillus terreus and Aspergillus glaucus
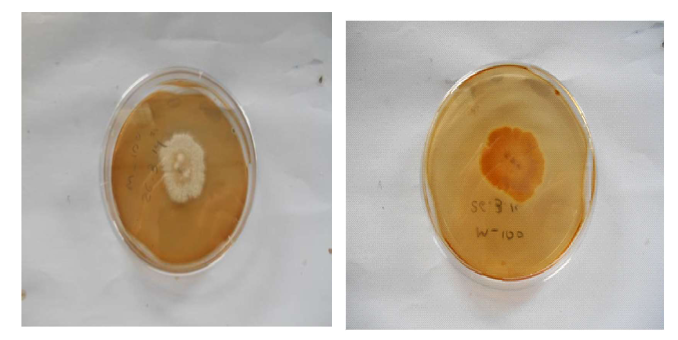
Plate 3(C) & (D) . Aspergillus terreus Front & Back view on Potato dextrose agar plate
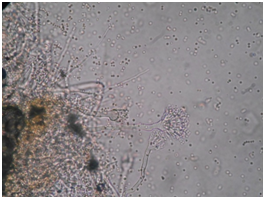
Plate 3 (E). Aspergillus terreus(400x)
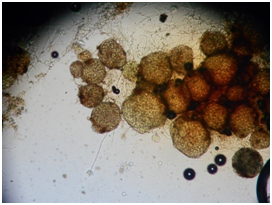
Plate 4. Aspergillus glaucus(400x)
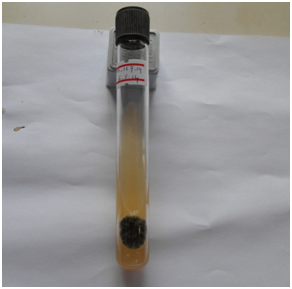
Plate 5(A). Cladosporium species on Sabouraud dextrose agar slant
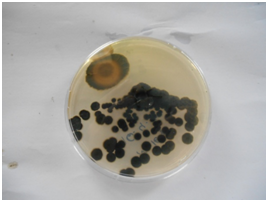
Plate 5(B). PDA
Plate 6 (A) & (B). Mucor species (Front & Back views) on Sabouraud dextrose agar slant
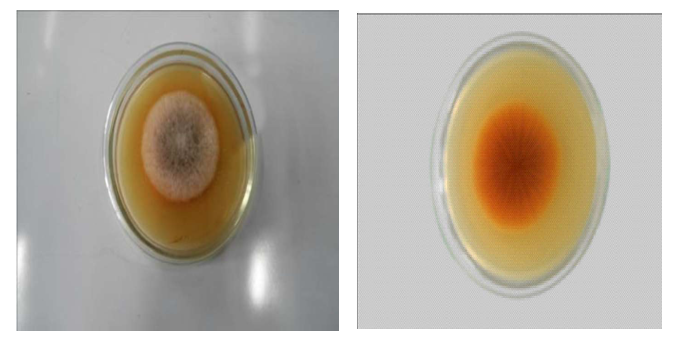
Plate 6(C) & (D). Mucor species (Front & Back views) on Potato dextrose agar
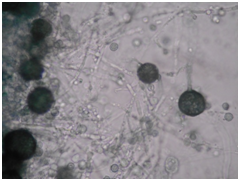
Plate 6(E). Microscopic appearance of Mucor species (LCB, 400X, OLM)
Plate 7 slide culture method

Plate 8. Growth of Candida albicans on Sabouraud dextrose agar with chloramphenicol.
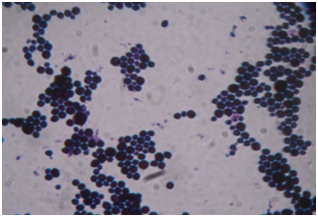
Plate 9. Gram-stained preparation of blastospores of Candida albicans from Sabouraud dextrose agar with chloramphenicol.
DISCUSSION
The ear can be divided anatomically and clinically into three parts: external ear, middle ear and internal ear. External ear and middle ear are concerned primarily with the transmission of the sound. Otomycosis or fungal external otitis is an acute, subacute or chronic infection produced by yeasts and filamentous fungi (Gutierrez et al., 2005).
Pathogens vary from temperate to tropical climates, but Candida species and Asperigillus species are common in both climates. Aspergillus species is the most common fungi that causes otomycosis and are environmental fungi. Another common causative agent of otomycosis is Candida albicans which is an endogenous microorganism commonly inhabiting the gastrointestinal and urogenital tracts ( Pradhan et al., 2003 ).
Aspergillus is rarely pathogenic in the normal host, but can produce disease in immunosuppressed individuals and patients treated with broad-spectrum antibiotics. The disease has a worldwide distribution. Aspergillus niger is commonly found as a saprophyte growing on dead leave, stored grain, compost piles, and other decaying vegetation. The spores are wide spread, and are often associated with organic materials and soil. Aspergillus niger, an opportunistic filamentous fungus, was identified as the cause of chronic unilateral otomycosis (Rutt and Sataloff, 2008).
Aspergillus flavus is a common contaminant in agriculture. It is widely distributed filamentous fungus that contaminates crops with the potent carcinogen aflatoxin (Mellon and Cotty, 2004).
Aspergillus terrus is an agent of allergic bronchopulmonary aspergillosis. Aspergillus glaucus is occasionally reported as infection of nails, ear, brain, and cardiovascular and visceral sites.
The clinical spectrum of manifestations by Candida ranges from superficial infections of the skin to systemic life-threatening infections (Murray et al., 2002).
Candida albicans is part of the normal human flora of the mouth, gastrointestinal tract, and vagina. Candida tropicalis is known to cause infection, especially in immunocompromised, predisposed patients. Candida parapsilosis is the second most common agent of fungal endocarditis. Candida guilliermondii has occasionally been reported to cause endocarditis, osteomylitis, cutaneous and urinary tract infections, and disseminated disease. Infection can be fatal in the immunocompromised patient. Cladosporium species are pigmented molds widely distributed in the air as well as decayed organic matter, and very often they are food contaminants. The genus Cladosporium includes over 30 species. The most common ones include Cladosporium cladosporioides, Cladosporium elatum, Cladosporium harbarum, Cladosporium sphaerospermum. Rhizopus and Mucor are ubiquitous saprophytes in soil and are commonly found on bread and many other foodstuffs. This fungus is also known as a common contaminant (Larone, 2011).
In the present study culture proved otomycosis was 83% (83 out of 100suspected cases) of these suspected patients.
The present study has the similar result as others studies. (Paulose et al., 1989; Degerli,et al , 2012; Jia ,et al , 2012; Panchal,et al , 2013; Moharram,et al , 2013); Sarvan,et al , 2012). Because Aspergillus niger grows on cerumen, epithelial scales and debris deep in the external auditory canal and resulting in plug of mycelium.
The results of the present study was comparable to that of Khin-Thu -Zar- Htwe in which 67.08 % (53/124) of the isolates was Aspergillus niger followed by Aspergillus flavus 16.45 % (n=13), Aspergillus fumigatus 6.33% (n=5), Aspergillus terreus 3.79% (n=3) and Candida parapsilosis 6.33% (n=5).
However, a study conducted in Iran showed that otomycosis was diagnosed in 8 (11.4%) of 70 investigated patients and Candida species was the most frequent: Candida parapsilosis (5 cases), Candida glabrata (2 cases) and Candida krusei (1 cases) (Bineshian et al., 2006).
Variation from the findings of other investigators might be attributable to differences in population groups, habits, climatic conditions, and methods of isolation.
Similar to the present study where Cladosporium species, a rare fungus, was detected in 2 out of 83 culture positive ( 2.40%) Moharram,et al (2013) showed that the incidence of Cladosporium species was 2.2% (in 2 out of 92 cases mycologically positive patients).
Yangon has a tropical monsoon climate with a lengthy rainy season from May to October and a dry season from November to April with little rainfall . The hot and humid environment of favors a high incidence of otomycosis, especially in patients with ear discharge.
Knowledge concerning the types of fungus causing otomycosis is essential for the effective control of otomycosis since variations in types of dominant fungus and their susceptibilities exist.
This study showed the prevailing fungal pathogens of otomycosis. Among the fungal causal agents, Aspergillus (mainly Aspergillus fumigatus) is the major causal agent of invasive external otitis (necrotizing or malignant otitis externa) with local spread to bone and cartilage, which can be a severe and potentially life- threatening diseases.
REFERENCES
- Desai K.J, Malek S.S, Italia I.K, Jha S, Pandya V and Shah H. (2012) Fungal Spectrum In Otomycosis At Tertiary Care Hospital. National Journal Of Integrated Research in Medicine, 3(5): 58-61
- Gutiérrez P.H, Álvarez S.J, Sañudo E. C. G, A V García L. M .G, Sánchez C. R and Valdezate I. (2005) Presumed diagnosis: Otomycosis. A study of 451 patients. Acta Otorhinolaryngologica Espanola; 56: 181- 186.
- Booth J.B. (1987) Otology. In: Scott-Brown’s Otolaryngology, 5th edition, (Ed: Alan G Kerr) Butterworth and Co (Publishers) Ltd, p.167.
- Mogadam A.Y, Asadi M.A, Dehghani R and Hooshyar H. (2009) The prevalence of otomycosis in Kashan, Iran during 2001-2003. Jundishapur Microbiology; 2(1): 18-21
- Howard B.J, Keiser J.F and Weissfeld A.S. (1994) Clinical and Pathogenic Microbiology, 2nd edition, St Louis, Mo; Mosby-Year Book.
- Forbes B.A, Sahm D.F and Weissfeld A.S. (1998) Infections of the urinary tract. In: Bailey and Scott’s Diagnostic Microbiology, 10th edition; Mosby Inc; pp. 350-362.
- Larone D.H. (2011). Medically Important Fungi, In: A Guide to Identification, 5th edition, American Society for Microbiology, Washington D.C., U.S.A: pp. 177-292.
- Gutiérrez P.H, Álvarez S.J, Sañudo E. C. G, A V García L. M .G, Sánchez C. R and Valdezate I. (2005) Presumed diagnosis: Otomycosis. A study of 451 patients. Acta Otorhinolaryngologica Espanola; 56: 181- 186.
- Pradhan B, Tuladhar N.R and Amatya R.M. (2003) Prevalence of Otomycosis in out patients department of otolaryngology in Tribhuvan University of Teaching Hospital, Kathmandu, Nepal. Ann Otol Rhinol Laryngol,112(4): 384-385.
- Rutt A.L and Sataloff R.T (2008) Aspergillus otomycosis in an immunocompromised patient. Ear Nose Throat Journal, 87(11): 622-3.
- Mellon J.E and Cotty P.J. (2004) Expression of pectinase activity among Aspergillus flavus isolates from southwestern United States. Mycopathologia, 157: 333-338
- Murray P.R, Rosenthal K.S, Kobayashi G.S and Pfaller M.A. (2002) Chapter 71. Opportunistic Mycoses, In: Medical Microbiology. 4th edition. U.S.A: pp. 671-672.
- Larone D.H. (1993) Medically Important Fungi, In: A Guide to Identification, 2nd edition, American Society for Microbiology, Washington D.C, U.S.A: pp. 146-147 .
- Paulose K.O, Khalifa A.L, Shenoy P and Sharma R.K (1989) Mycotic Infection of ear. The Journal of Laryngology and Otology, 103(1): 30-35.
- Panchal P, Pethani J, Patel D, Rathod S and Shah P. (2013) Analysis of various fungal agents in clinically suspected cases of otomycosis. Indian Journal of Basic & Applied Medical Research; 8(2): 865-869.
- Moharram A.M, Ahmed H.E and Nasr S A- M. (2013) Otomycosis in Assiut, Egypt. Journal of Basic & Applied Mycology (Egypt), 4: 1-11.
- Jia X, Liang O, Chi F and Cao W. (2012) Otomycosis in Shanghai: aetiology, clinical features and therapy. 55(5): 404-409.
- Sarvan R.R, Kikani K.M, Mehta S.J and Joshi P.J (2012) Clinico – mycological study of otomycosis. International Journal of Biological and Medical Research. 3(4): 2469-2470.
- Khin-Thu-Zar-Htwe (2006). Fungal Profile and Antifungal Susceptibility Patterns of Otomycosis in Mandalay. A thesis submitted for the degree of Master of Medical Science (Microbiology), University of Medicine, Mandalay.
- McGinnis M.R. (1980) Yeast identification.In Laboratory Handbook of Medical Mycology. Academic Press, Inc: pp. 350-375.
- Odds F.C (1979) Candida and Candidiosis. Leicester University Press: pp. 1-227.
Author Information
- Demonstrator,Department of Microbiology, University of Medicine 2, Yangon.
- Head, Mycology Section, National Health Laboratory, Yangon.
- Postgraduate Lecturer, Department of Microbiology, University of Medicine 2, Yangon.
- Postgraduate Lecturer, Department of Microbiology, University of Medicine 2, Yangon.
- Professor and Head, Department of Microbiology, University of Medicine 2, Yangon.


