Summary
Synchronous primary malignancies arising from different organs are uncommon and present diagnostic and therapeutic challenges. Gastric carcinoma frequently coexists with other gastrointestinal malignancies; however, the synchronous occurrence of gastric cancer and gallbladder carcinoma is rare. We report the case of a 75-year-old monk who presented with dyspeptic symptoms and weight loss and was diagnosed with gastric adenocarcinoma. During surgery, an incidental gallbladder tumor was discovered. Histopathological examination confirmed two distinct primary malignancies: moderately differentiated gastric adenocarcinoma and papillary adenocarcinoma of the gallbladder. The patient underwent partial gastrectomy with gastrojejunostomy and cholecystectomy with an uneventful postoperative recovery. This case highlights the importance of careful intraoperative evaluation and histopathological examination in detecting synchronous primary malignancies.
Introduction
The occurrence of multiple primary malignancies has been increasingly reported due to improvements in diagnostic modalities and prolonged patient survival. Multiple primary cancers may be classified as synchronous when diagnosed simultaneously or within six months of each other, and metachronous when they occur after a longer interval.
Synchronous malignancies involving the gastrointestinal tract are uncommon. Gastric cancer has been reported to coexist with malignancies of the colon, pancreas, and esophagus. However, the synchronous occurrence of gastric carcinoma and gallbladder carcinoma is rare. Recognition of such cases is important because management strategies and prognosis may differ from those of single primary malignancies.
We present a case of synchronous gastric and gallbladder carcinoma discovered in a 75-year-old monk who presented with symptoms suggestive of gastric pathology.
Case Presentation
A 75-year-old monk presented with burning sensation at the epigastrium for three months, associated with loss of appetite and weight loss. He also reported intolerance to solid food and habitual constipation. There was no history of vomiting or abdominal distension. He had no known underlying medical illnesses and was an ex-smoker.
Clinical Examination
On physical examination, the patient was in fair general condition with pallor present but no jaundice. Cardiovascular and respiratory examinations were unremarkable. Abdominal examination revealed a soft abdomen with no palpable mass, no visible peristalsis, and normal bowel sounds.
Investigations
Ultrasonography of the whole abdomen demonstrated: Mild fatty liver with no space-occupying lesion Tiny gallbladder stones and sludge Gallbladder wall thickness of approximately 4 mm Gastric wall thickening suspicious for gastric carcinoma or chronic gastritis. Upper gastrointestinal endoscopy (OGDS) was performed on 23 May 2017, revealing an ulcerated growth near the pylorus without active bleeding. Histopathological examination of the biopsy confirmed moderately differentiated adenocarcinoma of the prepyloric region of the stomach.
Surgical Management
The patient underwent partial gastrectomy with gastrojejunostomy and cholecystectomy on 2 June 2017.
Intraoperative Findings
Liver surface smooth No peritoneal deposits No ascites Gallbladder growth identified intraoperatively
Procedure
Cholecystectomy was performed due to the presence of a palpable gallbladder lesion. The duodenal stump was divided using a 75-mm linear stapler. Partial gastrectomy was performed using a stapling device. Gastrojejunostomy was constructed approximately 30 cm distal to the duodenojejunal junction. Peritoneal toileting and drain placement were performed. A nasogastric tube was positioned within the afferent loop.
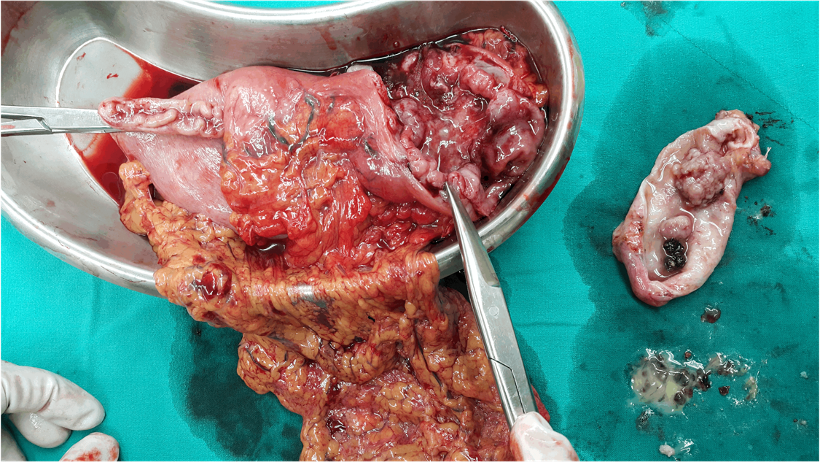
Fig.1– Partial gastrectomy and gallbladder specimens
Histopathological Findings
Histopathological examination revealed two separate primary malignancies:
Stomach
Diffuse moderately differentiated adenocarcinoma Tumor infiltration involving the circumferential margin and serosa Proximal and distal resection margins free of tumor Gastric lymph nodes showed reactive follicular and sinus hyperplasia
Gallbladder
Polypoid papillary moderately differentiated adenocarcinoma Superficial muscular invasion Associated chronic cholecystitis
These findings confirmed the diagnosis of synchronous primary malignancies of the stomach and gallbladder.
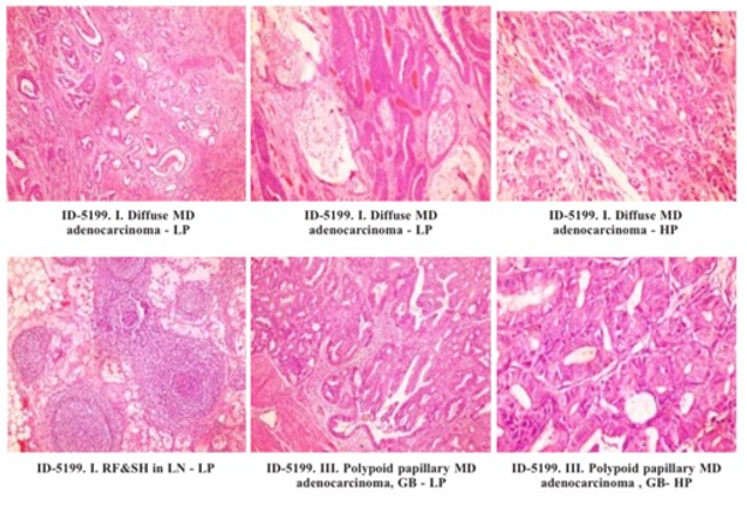
Fig.2– Histopathological slides of gastric and gallbladder specimens
Postoperative Course
The patient had an uneventful postoperative recovery. He was discharged on postoperative day 7, and skin staples were removed on postoperative day 11. No postoperative complications were reported.
The patient subsequently received adjuvant oncological treatment of oral chemotherapy Xeroda (Capecitabine) 500mg BD 2 weeks course was given for 2 cycles. However, the patient defaulted oncology follow up since then. The patient survived for six years following surgery before succumbing to disease progression.
Discussion
Synchronous multiple primary malignancies are defined by the Warren and Gates criteria, which require that each tumor be malignant, histologically distinct, and not represent metastasis from another primary tumor. 1
The coexistence of gastric and gallbladder carcinoma is extremely uncommon.2
Several factors have been proposed to explain synchronous gastrointestinal malignancies, including:
Environmental carcinogens Chronic inflammation Genetic susceptibility Field cancerization phenomenon Shared risk factors such as smoking and dietary habits
In the present case, the gallbladder carcinoma was discovered incidentally during surgery. Preoperative imaging only demonstrated gallstones and mild gallbladder wall thickening, illustrating the limitations of ultrasonography in detecting early gallbladder carcinoma.
Contrast-enhanced computed tomography (CECT) could have potentially provided better preoperative staging and detection of additional malignancies. CECT plays a crucial role in:
Tumor staging Evaluation of regional lymph nodes Detection of distant metastasis Identification of synchronous malignancies
Management of synchronous cancers depends on tumor stage and patient condition. In this patient, simultaneous resection of both malignancies was feasible and appropriate, allowing definitive treatment in a single surgical procedure.
Postoperative management should include oncology consultation for adjuvant therapy, particularly for gastric carcinoma with serosal involvement.
Conclusion
Synchronous gastric and gallbladder carcinomas are rare and may be discovered incidentally during surgical exploration. Thorough intraoperative assessment and careful histopathological examination are essential for diagnosis. Preoperative imaging such as CECT may improve detection of additional malignancies. Early recognition and simultaneous surgical management can lead to favorable outcomes.2, 3
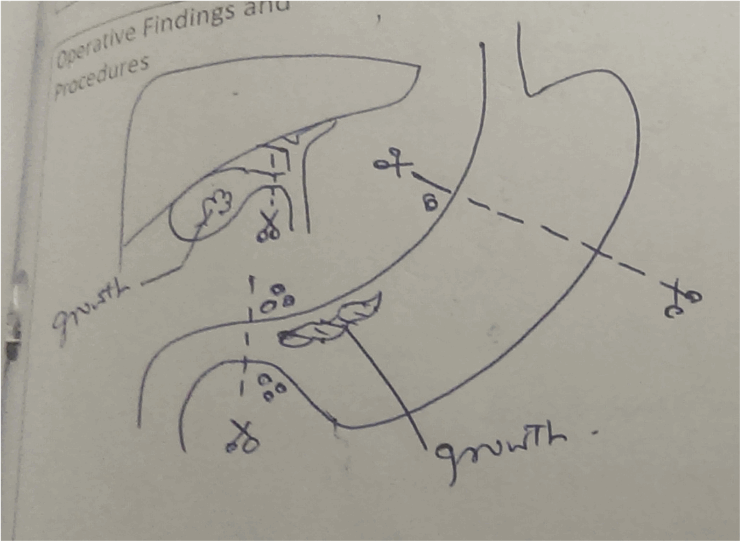
Fig.3-Scratch drawing of partial gastrectomy and cholecystectomy operation notes

Fig.4– The patient with upper midline laparotomy Post Op Day 3
Reference:
- Warren S, Gates O. (1932) Multiple primary malignant tumors: a survey of the literature and statistical study. Am J Cancer.;16:1358 –1414. ¬¬
- Li Y, Wang J, Zhang X, et al. (2017) Synchronous multiple primary gallbladder and gastric malignancies: Report of two cases and review of the literature. Oncol Lett.;14(5):6083–6088.
- Kato M, Tsuji T, Sugiyama H, et al. (1987) Synchronous early double cancers of the stomach and gallbladder. Gan No Rinsho ;33(9):1095–1100. PMID: 3626038.
Author Information
Myo Kyi1, Aung Moe Hlaing2, Soe Naung Win3, Ko Ko Zeyar Toe4, Maung Maung Oo5 and Professor Win Myint6
(1) Consultant General Surgeon, Pun Hlaing Hospitals, Yangon
(2) Consultant General Surgeon, Pun Hlaing Hospitals, Yangon
(3) Consultant General Surgeon, Pun Hlaing Hospitals, Yangon
(4) Surgical Registrar, Pun Hlaing Hospitals, Yangon
(5) Surgical Resident, Pun Hlaing Hospitals, Yangon
(6) Senior Consultant Surgeon, Pun Hlaing Hospitals, Yangon