A 48-years-old woman was referred to us from a private hospital to confirm OSAS by sleep study.
The patient complained of inability to sleep in the supine position (usually slept in the upright position), loud snoring (reported by her relatives), sleep interruption and excessive daytime sleepiness.
She was under care by consultants from multiple domains for hypertension, type 2 diabetes, osteoarthritis both knees and had taken multiple medications for her comorbidities.
She denied history of COPD, stroke or other neuromuscular conditions.
On examination, morbid obesity (BMI=54.25 Kg/M2) was noted, short and thick neck with Mallampati score class 4, no enlarged palatine tonsil and mild bilateral pedal oedema. BP before the test was 120/70mmHg with pulse rate =80/min and normal heart sounds.
Chest x-ray revealed cardiomegaly with no specific mention of lungs, pathology and echocardiogram report showed left ventricular enlargement with mild TI and EF= 55%.
Serum bicarbonate level was 29 mmol/L, raised serum urate, plasma lipids and normal thyroid function profile. Renal, metabolic and liver profile were unremarkable.
Vital signs were all within normal limit apart from ETCO2= 66 mmHg detected by side stream patient’s monitor (10 min sustained during awake) just before sleep test. Her pretest SpO2 level was 97% and ESS (Epworth Sleepiness Scale) was recorded 15 (Ref;>10=sleepy patient).
Level -1 overnight sleep study was performed on Aug 9, 2025, from 23;01;00 h to D 7;24;00 h.
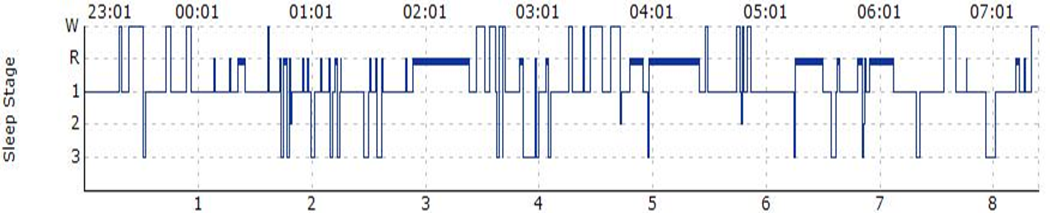
Fig. 1-Hypnogram from the patient by level-1 PSG (EEG + EOG+EMG multiple channels).
W=Wake, R= REM sleep 1= NREM1, 2= NREM2, 3= NREM (3+4) and Latency to REM sleep was 68.0min.
AHI= 59.3/hr , ODI= 38.1/hr Minimal SpO2 (Nadir)= 51% ETCO2 10 min sustain before sleep test = 66mmHg by side stream monitor. Multiple fragmentation sleep patten were also noted.

Fig. 2– SpO2 trend recorded from the patient during overnight sleep test. T90 or Time below 90% SpO2 fall was recorded 31.8% of total sleep time.
Our final diagnosis was OHS (Obesity Hypoventilation Syndrome, OSA dominant phenotype) with multiple comorbidities. We referred the patient back to her family physician.
Diagnostic criteria
1- Obesity = BMI= 54.25 Kg/M2(class=4 obesity).
2- ETCO2 (surrogate for PaCO2 by ABG) = 66 Hg at day time awake period (10 min sustained) or evidence of hypoventilation.
3- Serum bicarbonate level= 29mmo/L (cut off level=27mmol/L for OHS).
4- Patient symptoms of seep disordered breathing at night and abnormal day time sleepiness after wake up (ESS=15).
5- clinically excluded other possible causes of hypoventilation.
The history of its naming and evolution of OHS
It is previously known as Pickwickian Syndrome. In 1836, a novel “The Posthumus paper of the Pickwick Club” written by a famous British author Charles Dickens had many characters in his novel including Mr. Pickwick, owner of the club who did not suffer SBD symptoms. But the club servant and a character, Joe the fat boy ate a lot and always sleepy both day and night. In 1956, the condition was given to patients with chronically sleepy character, like Joe the fat boy. This was a misnomer and the syndrome did not differentiate between OHS and OSA. Since 1960, various studies can differentiate between OHS and OSA, the term “Pickwickian Syndrome” was no longer used.
Fig.3-Charles Dickens, the Pickwick club from a novel of Pickwick papers and sleepy Joe.
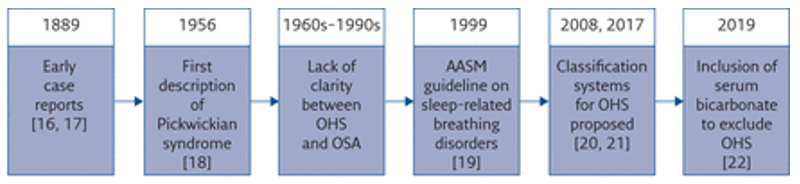
Fig. 4-Evolution of the identification OHS coded from AASM.
Current definition of OHS
OHS is defined by the combination of obesity (BMI>30Kg/M2), sleep disordered breathing and daytime hypercapnia (PaCo2>45mmHg at sea level) during wakefulness occurring in the absence of alternative neuromuscular, machinal or metabolic explanation of hypoventilation (ERS1). By definition, this condition is a diurnal pathology (day time pathology).
At night, more hypercapnia level can be expected due to effect of sleep on respiratory mechanism. Concomitant hypoxia may or may not be present.
American Academy of Sleep Medicine (AASM) arbitrarily defined sleep hypoventilation by the following criteria-
PaCo2 (or surrogate ETCO2 or TCCO2) >55mmHg for 10 minutes or increased in PaCO2 level (or surrogate) > 10mmHg compared to supine awake value to a value of 50mmHg for > 10 minutes.
Nearly 70% of OHS patients have concomitant severe OSA(AHI>30/hr) and remaining have non obstructive hypoventilation with no or mild OSA.
Epidemiology
Prevalence significantly varies across studies, current estimate of OHS between 8% and 20% of obese population referred to sleep centers. Most patients usually admitted to emergency department for treatment of acute on ch; respiratory failure. OHS was diagnosed during or after hospital stay when the patients were referred to sleep testing procedure.
Underlying pathophysiology
Day time hypercapnia is usually explained by many coexisting mechanisms such as obesity related changes in respiratory system, alteration in respiratory drive and breathing abnormalities during sleep (REM dependent hypoventilation) 1
Clinical presentations;
Acute on chronic hypercapnic respiratory failure. Usually mistaken as obstructive airway diseases or type 2 respiratory failure and delayed in actual diagnosis for years.
Comorbidities in an OHS patients
OSA (up to 70% have severe disease, AHI >30/h), Hypertension, pulmonary hypertension (50%), CAD, CHF and other cardiometabolic diseases.
International diagnostic criteria of OHS
ICSD -3 diagnostic criteria 4
Criteria A to C must be met.
A- Awake hypoventilation, PaCO2>45mmHg (EtCO2/TcCO2 as surrogate).
B- BMI>30Kg/M2 or >95th % of age or sex in children.
C- Exclusion of other causes of hypoventilation; lung parenchyma, vascular or airway pathology, neuromuscular diseases and primary central alveolar hypoventilation syndrome.
Note,
1-PSG shows worsening of hypoventilation during sleep
2- If OSA is present diagnosis of both OSA and OHS should be made.
3- Arterial O2 desaturation is usually present, but is not required for OHS diagnosis.
The definitive test to OHS was ABG test (for hypercapnia) at room air to an obese patient with SBD signs and symptoms, but it is not always available and inconvenient to patients sometimes.
Serum bicarbonate role in screening of OHS
Serum HCO3< 27 mmol/L = negative predictive value for OHS=96%
Serum HCO3 >27 mmol/L= Positive predictive value= 69% then proceed to ABG to check PaCO2. Both have sensitivity (92%) and specificity (50%).
Exclusion of other causes of raised serum HCO3 level must be done; eg. severe vomiting, dehydration, medications etc.
Role of sleep test
Overnight Polysomnogram is required to detect severe OSA (OSA dominant phenotype and PAP titration and recommendation) or to exclude non-obstructive hypoventilation phenotype (sleep hypoventilation dominant) to decide on NIV treatment.
Differential diagnosis of OHS
Central sleep apnea, COPD, neuromuscular diseases, chest wall restrictive diseases, myasthenia gravis, Guillain-Barre’ syndrome, myxedema and poliomyelitis should be excluded.
OHS Phenotypes
OSA dominant (AHI>30/hr) or hypoventilation dominant types (AHI<30/hr or no OSA).
Proposed severity classification in OHS patients
Recent OHS researches and trials suggest severity matrix for OHS.
Stage I – obesity-associated sleep hypoventilation – BMI >30 kg/m2, coexisting OSA or hypoventilation during sleep with intermittent hypercapnia during sleep and serum bicarbonate level <27 mmol/L during wakefulness;
Stage II – obesity-associated sleep hypoventilation – BMI >30 kg/m2, coexisting OSA or hypoventilation during sleep with intermittent hypercapnia during sleep, but with serum bicarbonate level ⩾27 mmol/L during wakefulness;
Stage III – obesity hypoventilation – BMI >30 kg/m2, with coexisting OSA or hypoventilation during sleep, and sustained hypercapnia during wakefulness;
Stage IV – obesity hypoventilation syndrome – BMI >30 kg/m2, daytime hypercapnia (PaCo2 ⩾45 mmHg) and sleep-disordered breathing/hypoventilation, cardiometabolic comorbidities (subject to excluding other disorders that may cause alveolar hypoventilation).
Management of OHS
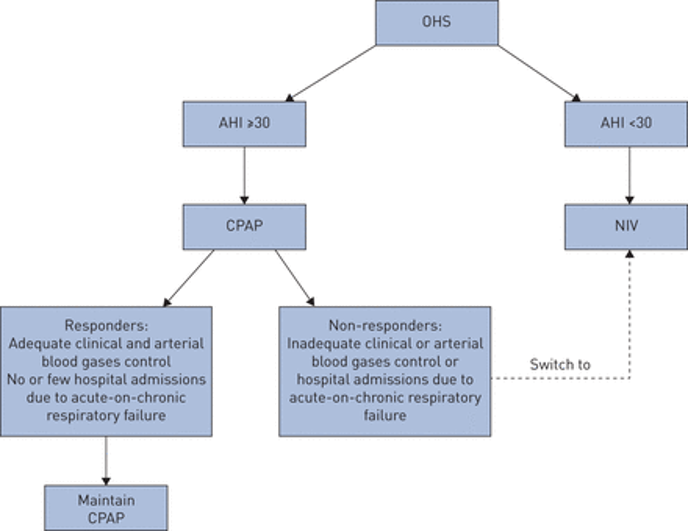
Fig. 5-Management of OHS adopted from ERS OHS review article 3.
At first OHS” phenotype” should be taken into consideration of individual patient management mainly PAP section mode.
CPAP treatment outcome
CPAP and life style modifications improve daytime sleepiness, day time PaCO2 (PAP compliance patients), serum HCO3 level, health related QOL compared to control group. Reduction in hospital resources utilization was reported after 5 years prior to treatment.
NIV outcome
Studies showed improvement in day time awake PaCo2 and PaO2 level, health related QOL, respiratory parameters (FEV1, FVC, 6 minutes’ walk distant ect) compared to life style modification group(control).
Also has potential for reduction in pulmonary arterial pressure in patient with pulmonary hypertension and left ventricular hypertrophy.
Another PAP mode Volume targeted pressure support outcome (AVPS, Asure Volume Pressure Support)
This PAP mode ensures variable PAP mode to support tidal volume along with pressure support to the patients especially during change in body positions and sleep stages (effective control of SBD) contrast to fixed pressure setting (IPAP and EPAP) in bilevel pressure mode. But it is important to consider not to disturb patient’s sleep due to high volume and pressure setting.
New PAP mode, Intelligent Volume assured Pressure Support outcome (IVAPS);
This is a new PAP mode to enhance ventilator adherence. Reported safe and effective in medium term management to OHS patients compared to fixed bilevel PAP mode.
The current data suggested no clear clinical benefit among each model and clinician should carefully consider their role when individualizing patients care.
Non-PAP management in OHS patients
Diet, exercise, life style change and rehabilitation program are good for short term gain, but do not sure about long term body weight control and clinical outcome. Targeted bod weight deduction is 25-30% to improve hypoventilation.
Bariatric surgery; a good strategy for severe obesity with comorbidity (eg-OSA) management, but the risk of surgery is very high in untreated OHS patients. No reliable data is available regarding long benefit or complication of bariatric surgery.
Newly approved drug like GLP-1 receptor agonist and combination formula with GIP, along with restricted calory intake and physical exercise can help body weight reduction and improving SBD symptoms.
Respiratory stimulant such as such as medroxyprogesterone and acetazolamide did not have established role in treating OHS patients.
Recombinant human leptin (metreleptin) is also not studied for OHS.
Supplemental O2 therapy may be required in OHS patient along with PAP devices when PAP mode alone cannot improve hypoxia.
But giving O2 therapy alone is “strongly discouraged” as it does not improve ventilation and even worsen CO2 retention.
Tracheostomy
To consider only for those intolerants of or consistently non-adherent to PAP therapy, or those with complications such as cor pulmonale. The OHS patients still need PAP therapy after tracheostomy as the procedure primarily solves upper airway obstruction and does not modify underlying pulmonary mechanics, ventilatory drive, or neurohumoral pathophysiology.
Prognosis OHS patients
Several studies reported 1 yr mortality of 18% (55% with PAP treatment). Mortality rate of 24% after 1.5 to 2 years and 31.3% after 3 years (unknown No. with PAP treatment)
References
- Mokhlesi B, Kryger MH, Grunstein RR.(2008) Assessment and management of patients with obesity hypoventilation syndrome. Proc Am Thorac Soc; 5: 218–225.
- Juan F. Masa etal, (2019) Obesity hypoventilation syndrome, European Respiratory Review, 28(151): 180097.
- Kania A etal, (2025) staging obesity hypoventilation patients who undergo bariatric surgery, Chron Respir Dis; Apr 25;22:14799731251338269
- ICSD3 International classification of Sleep Disorders and Diagnostic AASM,2014
- Obesity hypoventilation syndrome, update (2025) stat pearls National Institute of Health.
- Masa JF, Corral J, Alonso ML, et al. (2015) Efficacy of different treatment alternatives for obesity hypoventilation syndrome. Pickwick Study. Am J Respir Crit Care Med; 192: 86–95
Author Information
Zay Ya Aye
MBBS, MMed, Sc. Internal Medicine