Kyaw Linn
Introduction
Hyperactivity is one of the most frequent behavioural concerns encountered in paediatric practice. Parents may describe the child as “always moving”, “unable to sit still”, “too active”, “impulsive”, “difficult to control”, or “not listening”. Teachers may report difficulty remaining seated, interrupting, poor task completion, disruptive behaviour, or difficulty following classroom routines.
Hyperactivity is not a diagnosis. It is a behavioural presentation that may reflect normal developmental variation, temperament, environmental mismatch, emotional distress, sleep disturbance, neurodevelopmental disorder, systemic illness, medication effect, or, less commonly, neurological disease. The key clinical challenge is to distinguish a normally active child from a child whose activity level is developmentally inappropriate, persistent, impairing, unsafe, or secondary to an underlying condition.
The most recognised neurodevelopmental condition associated with hyperactivity is attention-deficit/hyperactivity disorder (ADHD). However, ADHD should not be diagnosed simply because a child is active or disruptive. Diagnosis requires a broad clinical and psychosocial assessment, developmental history, information from more than one setting, evidence of functional impairment, and consideration of coexisting or alternative conditions.
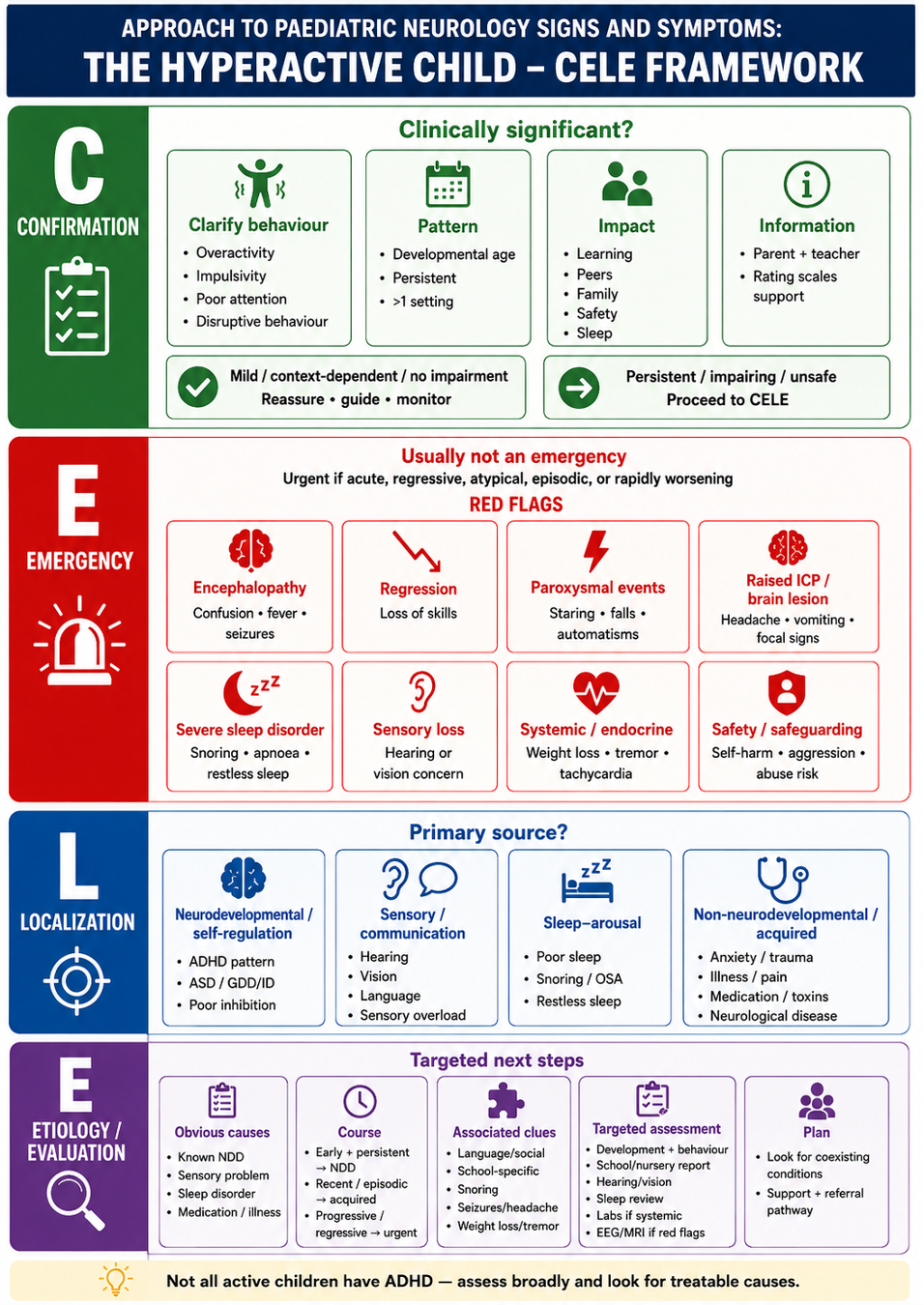
This article uses the CELE framework – Confirmation, Emergency, Localization, and Etiology – to provide a structured approach to children presenting with hyperactivity. The aim is to confirm whether hyperactivity is clinically significant, identify urgent or serious causes, ocaliza the likely source of the behaviour, and guide proportionate assessment, referral, and management.
Overview
Activity, curiosity, impulsivity, and short attention span are common in childhood, particularly in toddlers and preschool children. These behaviours are usually context-sensitive and may improve with maturation, structure, consistent routines, adequate sleep, responsive parenting, and developmentally appropriate expectations.
The clinical threshold for concern is functional impact. Hyperactivity becomes clinically significant when it interferes with home routines, school participation, learning, peer relationships, safety, emotional wellbeing, or family functioning. A child who is active but learning, ocalizatio, sleeping, and functioning well may need reassurance and monitoring rather than diagnostic assessment. In contrast, persistent and impairing hyperactivity requires structured evaluation.
Although ADHD is an important cause, hyperactivity may also occur with autism spectrum disorder, global developmental delay, intellectual disability, developmental language disorder, learning disorder, developmental coordination disorder, sensory impairment, sleep disorder, emotional distress, systemic illness, medication effects, toxin exposure, or acquired neurological disease.
Therefore, the hyperactive child should be approached as a child with a developmental, behavioural, medical, and psychosocial presentation, rather than as a child with a presumed diagnosis.
C – Confirmation of Clinically Significant Hyperactivity
The first step is to confirm whether the behaviour is clinically significant or represents normal developmental activity, temperament, environmental mismatch, or a transient response to stress, poor sleep, illness, medication change, or situational demands. Excessive movement alone is not enough to justify a diagnostic label or extensive assessment.
Confirmation should focus on whether the activity level is developmentally inappropriate, persistent, pervasive, and functionally impairing. The aim at this stage is not to diagnose ADHD, but to decide whether the concern is significant enough to proceed to structured developmental, behavioural, educational, or medical assessment.
A careful history should clarify what caregivers and teachers mean by “hyperactive”. The clinician should translate the label into observable behaviours such as constant movement, fidgeting, climbing, excessive talking, impulsive actions, difficulty waiting, emotional outbursts, poor attention, non-compliance, or disruptive behaviour.
The behaviour should be interpreted against the child’s developmental age, not chronological age alone. This is particularly important in children with developmental delay, language disorder, autism spectrum disorder, intellectual disability, or learning difficulty, where expectations may exceed the child’s actual developmental capacity.
The duration, course, and setting should be established. Persistent symptoms across months and across more than one setting are more concerning than brief or context-specific behaviour. Sudden onset or clear deterioration from baseline should raise concern for acquired emotional, medical, or neurological causes.
Functional impact should be assessed explicitly. Important areas include learning, play, peer relationships, family life, safety, self-care, sleep, and participation in age-appropriate activities. A child who is active but functioning well may need reassurance and practical guidance. Hyperactivity associated with educational difficulty, peer rejection, unsafe impulsivity, family exhaustion, exclusion, or distress warrants further evaluation.
Information should be obtained from more than one source whenever possible, including parent report, teacher or nursery report, developmental records, schoolwork, behaviour logs, and clinical observation. Rating scales may support assessment but should not be used as the sole basis for diagnosis or referral decisions.
Confirmation is therefore a decision point. Mild, context-dependent, developmentally appropriate, and non-impairing hyperactivity may not need formal diagnostic assessment immediately. Persistent, pervasive, impairing, unsafe, or clinically concerning hyperactivity should proceed to the next steps of the CELE framework.
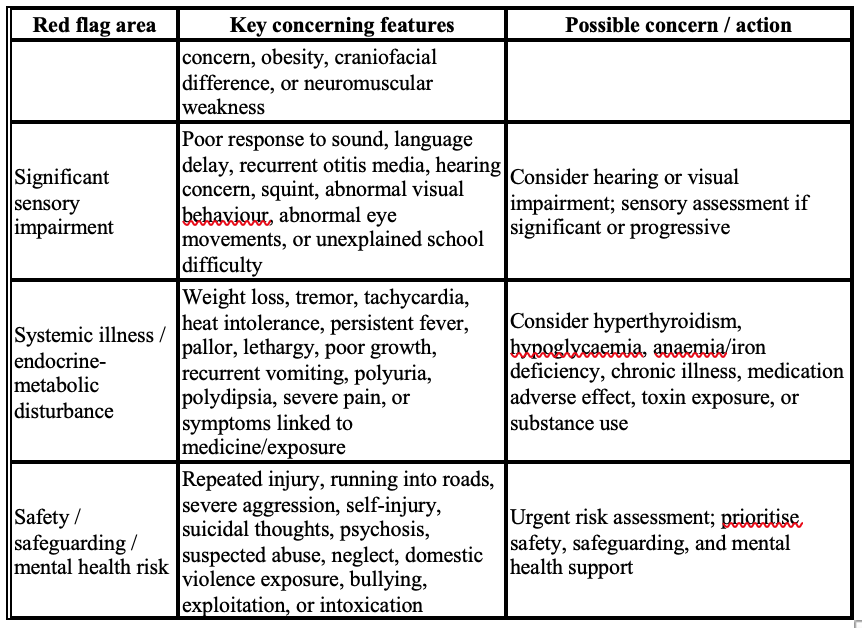
E – Emergency Considerations
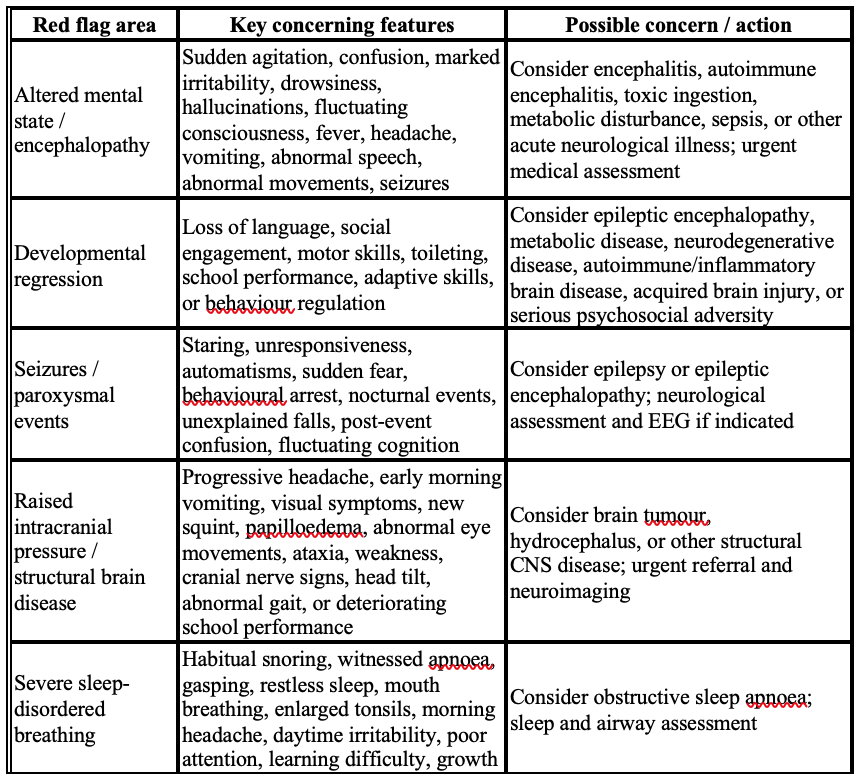
Hyperactivity is rarely a medical emergency in itself. Most children with excessive activity, impulsivity, or poor attention can be assessed through a structured developmental and behavioural pathway. However, apparent hyperactivity or behavioural dysregulation may occasionally be the first sign of a serious, treatable, or time-sensitive condition. Emergency consideration is particularly important when the behaviour is acute in onset, rapidly worsening, episodic, associated with regression, unsafe, or clearly different from the child’s previous baseline. In these situations, the priority is not to label the child as having ADHD, but to identify children who need urgent medical, neurological, mental health, sensory, sleep, or safeguarding assessment.
A child with long-standing, cross-situational hyperactivity and no red flags may proceed through routine developmental and behavioural assessment. In contrast, acute, progressive, atypical, regressive, unsafe, or medically concerning behavioural change requires urgent evaluation before routine diagnostic labelling.
L – Localization of the Primary Source of Hyperactivity
After clinically significant hyperactivity has been confirmed and urgent red flags have been considered, the next step is to ocaliza the primary source of the behavioural presentation. In this context, localization does not mean precise anatomical localization. Rather, it asks whether the hyperactivity mainly arises from :
- primary neurodevelopmental or self-regulation difficulty;
- sensory or communication-related difficulty;
- sleep–arousal disturbance; or
- non-neurodevelopmental or acquired conditions.
This step helps avoid assuming that all hyperactive behaviour represents ADHD and directs the next stage of assessment in a proportionate way.
Primary neurodevelopmental / self-regulation difficulty
This pattern is suggested when hyperactivity, impulsivity, inattention, poor task persistence, emotional dysregulation, or poor inhibition are persistent and occur across settings. ADHD is the most ocalizati condition in this group, but hyperactivity may also occur with autism spectrum disorder, global developmental delay, intellectual disability, developmental language disorder, learning disorder, or developmental coordination disorder.
Sensory or communication-related difficulty
Some children appear hyperactive, inattentive, or non-compliant because they cannot adequately access or understand the environment. Hearing impairment, visual impairment, language comprehension difficulty, sensory overload, or sensory-seeking behaviour may present with restlessness, poor listening, disruptive behaviour, or difficulty following instructions.
Sleep–arousal disturbance
Sleep problems are common and treatable contributors to hyperactivity. Children with poor sleep may present with overactivity, irritability, impulsivity, emotional outbursts, and poor attention rather than obvious daytime sleepiness. Snoring, mouth breathing, witnessed apnoea, restless sleep, delayed sleep onset, or worsening behaviour after poor sleep should prompt sleep assessment.
Non-neurodevelopmental or acquired conditions
This group includes emotional distress, anxiety, trauma, bullying, family stress, safeguarding concerns, systemic illness, pain, endocrine or metabolic disturbance, medication effects, caffeine or stimulant exposure, toxin exposure, and acquired neurological disease. It should be considered when hyperactivity is recent, episodic, rapidly worsening, context-specific, or clearly different from the child’s previous baseline.
E – Etiology / Evaluation for Underlying Cause
Once the likely source has been ocalizat, the next step is to identify the underlying cause. Evaluation should be guided by the ocalization pattern, age at onset, duration, course over time, associated developmental or medical features, and functional impact. The aim is not to investigate every child extensively, but to identify children who need targeted neurodevelopmental, sensory, sleep, medical, psychosocial, or neurological assessment.
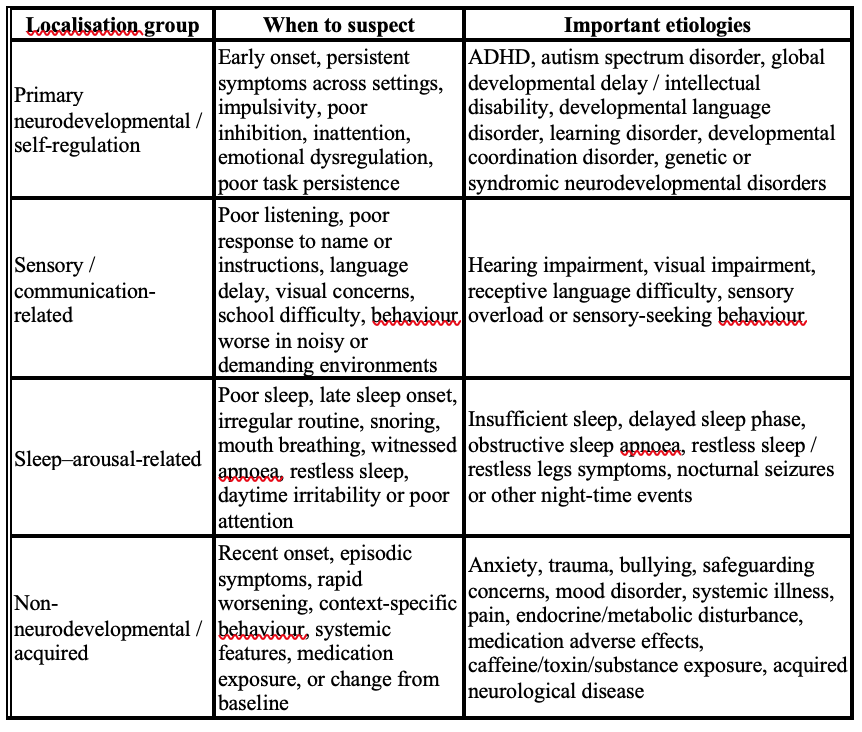
Etiology according to localisation pattern
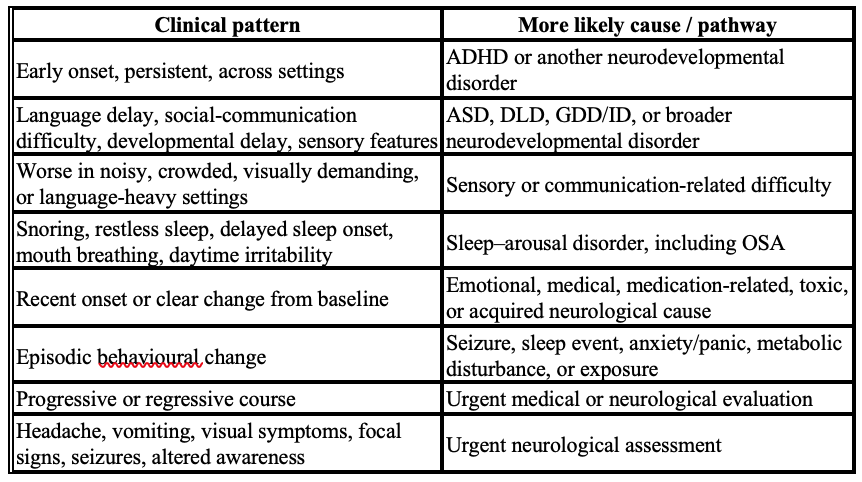
Key clinical patterns
ADHD should be considered when hyperactivity, impulsivity, and/or inattention are developmentally inappropriate, persistent, present in more than one setting, and associated with functional impairment. However, other neurodevelopmental disorders may produce similar behaviour when the child has difficulty with communication, learning, motor coordination, social understanding, adaptive functioning, or sensory regulation.
Sensory and communication difficulties should be considered when the child appears inattentive, restless, non-compliant, or disruptive because they cannot hear, see, process, or understand environmental information. Hearing impairment, visual impairment, receptive language difficulty, and sensory overload may all mimic or worsen hyperactivity.
Sleep-related causes are common and frequently overlooked. Insufficient sleep, delayed sleep phase, poor sleep routine, obstructive sleep apnoea, restless sleep, and nocturnal events may lead to daytime overactivity, irritability, impulsivity, and poor attention.
Non-neurodevelopmental or acquired causes should be considered when symptoms are recent, episodic, rapidly worsening, or associated with systemic, emotional, medication-related, toxic, or neurological features. Anxiety, trauma, bullying, safeguarding concerns, pain, constipation, eczema, asthma symptoms at night, anaemia, iron deficiency, endocrine or metabolic disturbance, medications, caffeine, toxins, and substance exposure may all contribute. Acquired neurological disease is uncommon but important when hyperactivity is associated with regression, seizures, altered awareness, abnormal movements, headache, vomiting, visual symptoms, ataxia, focal neurological signs, or personality change.
Clinical clues from duration and associated features
Aetiological evaluation should therefore be stepwise and targeted. This approach avoids assuming that all hyperactive children have ADHD, while ensuring that treatable developmental, sensory, sleep-related, medical, psychological, and neurological causes are not missed.
Conclusion
Hyperactivity is a common paediatric presentation, but it should be regarded as a clinical symptom rather than a diagnosis. Many children are active, impulsive, or restless as part of normal development, temperament, environmental mismatch, or temporary stress. The key clinical task is to identify when hyperactivity is developmentally inappropriate, persistent, pervasive, and functionally impairing.
A structured CELE-based approach provides a practical framework for assessment. Confirmation distinguishes clinically significant hyperactivity from normal variation or transient contextual behaviour. Emergency assessment identifies serious or treatable causes, particularly when hyperactivity is acute, progressive, regressive, episodic, unsafe, or associated with neurological, systemic, sensory, sleep, mental health, or safeguarding concerns. Localization identifies the likely source of the behavioural presentation, and etiological evaluation guides targeted assessment rather than indiscriminate investigation.
ADHD is an important and common cause of persistent hyperactivity, but it should not be assumed in every active child. The hyperactive child should be assessed through a broad developmental, behavioural, medical, educational, and psychosocial lens. This approach avoids premature labelling, supports early recognition of ADHD and other neurodevelopmental conditions, and ensures that treatable or time-sensitive causes are identified promptly.
References
- Wolraich ML, Hagan JF Jr, Allan C, Chan E, Davison D, Earls M, et al. (2019) Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics.;144(4):e20192528.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed, text revision. Washington, DC: American Psychiatric Association Publishing; 2022.
- Centers for Disease Control and Prevention. Diagnosing ADHD [Internet]. Atlanta: Centers for Disease Control and Prevention; 2026 Jun 1 [cited 2026 Jun 26]. Available from: https://www.cdc.gov/adhd/diagnosis/index.html
- Chan E. Attention deficit hyperactivity disorder in children and adolescents: clinical features and diagnosis [Internet]. In: Augustyn M, Tehrani N, editors. UpToDate. Waltham (MA): UpToDate Inc.; 2026 [updated 2026 May 22; cited 2026 Jun 26]. Available from: https://www.uptodate.com/contents/attention-deficit-hyperactivity-disorder-in-children-and-adolescents-clinical-features-and-diagnosis
- National Institute for Health and Care Excellence (NICE). Attention deficit hyperactivity disorder: diagnosis and management. NICE guideline NG87. London: National Institute for Health and Care Excellence; 2018. Updated 2019. Available from: https://www.nice.org.uk/guidance/ng87
Author Information
Kyaw Linn
Professor (Paediatric Neurology)
Senior Consultant Paediatrician