Thar Thar Oo
The management of acute hypertensive response (AHR) during the acute phase of stroke is a difficult decision-making process that has a direct impact on patient outcomes.
The goal of treating ischemic and hemorrhagic strokes is to balance the risks of cerebral hypoperfusion, hematoma expansion, and hemorrhagic transformation, sometimes concurrently.
Despite the fact that many studies have looked into the best blood pressure (BP) targets during the acute stroke phase, particularly following hemorrhagic stroke, a firm consensus is still elusive, and clinical practice frequently reflects a range of practice modalities, institutional protocols, and customized patient care.
AHR in Intracerebral Hemorrhage
The likelihood of hematoma extension, which happens most commonly in the first few hours following symptom start, is a major deciding factor in the well-established link between AHR and poor functional outcomes in individuals with intracerebral hemorrhage (ICH).
The idea that strong blood pressure lowering could prevent hematoma expansion and enhance functional outcomes was established by early research.
When to start lowering and how much to lower?
Within six hours of the onset of ICH, over 2800 participants in the pivotal Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage (INTERACT2) trial were randomly assigned to either a systolic blood pressure target of less than 140 mm Hg or a more permissive target of less than 180 mm Hg.
The trial results showed a trend toward better functional outcomes for people with systolic blood pressure of less than 140 mm Hg, even though the primary end point (death or major disability at 90 days) did not reach statistical significance.
According to secondary analyses, people who lowered their blood pressure significantly had higher health-related quality of life scores.
To improve these results, the Antihypertensive Treatment of Acute Cerebral Hemorrhage II (ATACH-II) experiment was created.
Even more stringent BP objectives were employed in ATACH-II, which randomly assigned >1000 participants to systolic BP targets of 110 to 139 mm Hg or 140 to 179 mm Hg within 4.5 hours of ICH onset. Renal adverse events were more common in the intensive treatment arm of the trial, but there was no discernible difference in 90-day morbidity or death between the groups.
These findings demonstrated the likely dangers of drastically lowering blood pressure, indicating a “low target” below which additional lowering could not be beneficial and might even be harmful, possibly by jeopardizing perihematomal perfusion in areas where cerebral autoregulation is compromised.
Additionally, more recent analyses have highlighted the significance of BP variability as opposed to just static thresholds.
Data from more recent observational cohorts and post hoc analysis of the INTERACT2 trial have repeatedly shown that variations in blood pressure, especially in the first 24 hours, are independently linked to worse outcomes, such as higher rates of hematoma expansion, neurologic deterioration, and 90-day mortality.
The majority of recent pooled analyses of both major trials show that the treatment focus for individuals with ICH has changed from a fixed systolic blood pressure target to emphasizing stability and avoiding fluctuation.
As a result, the use of short-acting intravenous (IV) medications (like clevidipine) and ongoing arterial blood pressure monitoring have become crucial elements of the best blood pressure management for people with ICH.
The purpose of the Clevidipine for the Antihypertensive Treatment of Acute Intracerebral Hemorrhage (CLUTCH) trial is to compare the percentage of patients with hypertensive ICH who can reach and sustain target SBP within 60 minutes of receiving IV clevidipine versus other IV antihypertensive medications. Enrollment for this trial is anticipated to conclude in the first half of 2026.
How about diastolic and mean arterial blood pressures?
The literature has not thoroughly examined the impact of diastolic blood pressure and mean arterial blood pressure on haematoma expansion and functional outcomes in ICH; one small randomized study that aimed for a mean arterial pressure of less than 115 mmHg did not demonstrate any improvement in functional outcomes. Because of this, current guidelines contain no recommendations regarding diastolic or mean arterial pressure targets.
How long?
Due to a lack of high-quality data, the ideal duration of acute blood pressure intervention in ICH is unknown.
The duration of the intervention was 24 hours in ATACH-2 and 7 days in INTERACT2 and INTERACT3.
Because of this, the European Stroke Organization’s guidelines are the only ones that address the duration of acute blood pressure management (24–72 hours), which was determined by expert consensus. It might be feasible to aim for the same systolic blood pressure target (less than 140 mmHg) after the first 24 hours, but with less aggressive interventions (i.e., oral rather than intravenous medications), since the majority of haematoma expansion happens in the first few hours following ICH.
Which agent?
Given the level of conscious state and acute dysphagia concerns in many ICH patients, intravenous agents are usually preferred. Nevertheless, the best medication or class of medications to regulate blood pressure is unknown and has not been thoroughly investigated in clinical trials.
Alpha-adrenergic antagonists, like urapidil (> 60% in INTERACT3), were the most frequently used agents, a drug that is rarely used in other settings. Local availability and practices influenced medication choice.
In the ATACH-2 trial, intravenous nicardipine was the first-line treatment, followed by intravenous labetalol.
It has been demonstrated that using nicardipine for 24 hours to control blood pressure during the hyperacute phase quickly lowers systolic blood pressure, which is associated with less hemorrhage expansion and improved functional outcomes.
Practically speaking, oral medication should be started as soon as patients are safe to swallow. Local availability, practicality, pharmacological profile, patient parameters (such as heart rate and renal function), potential side effects, and cost should all be considered. However, no guidelines specifically recommend an agent of choice. 1.8.7
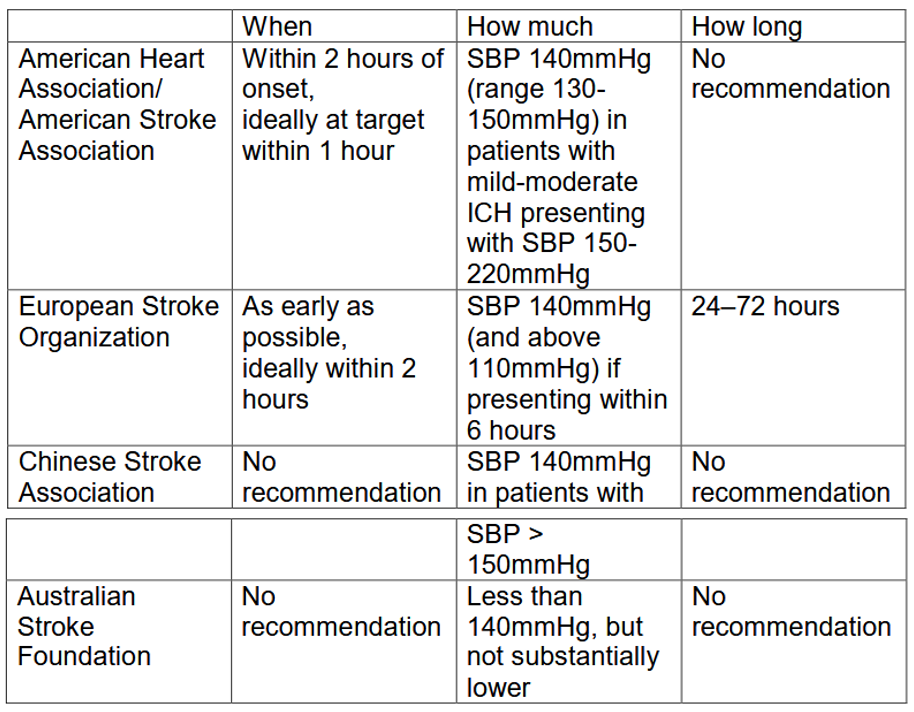
Table 1: Current stroke guideline recommendations regarding acute blood
pressure management in ICH.
AHR in Ischemic Stroke
Another level of complexity is the management of AHR in ischemic stroke patients, particularly when reperfusion demand is involved.
The ischemic penumbra frequently has impaired autoregulatory capacity, which makes the tissue susceptible to both hypoperfusion and hyperperfusion injuries. Autoregulatory capacity is the ability of an organ to maintain stable blood flow despite changes in perfusion pressure.
According to current guidelines, blood pressure should be kept at or below 180/105 mm Hg for at least the first 24 hours for patients undergoing IV thrombolysis (IVT).
This goal aids in striking a balance between the requirement to guarantee sufficient cerebral perfusion and the risk of hemorrhagic transformation.
The intensive BP target group had a lower incidence of any ICH, according to study results, but the primary outcome of disability or death at 90 days did not differ significantly. This emphasizes that aggressive blood pressure control should be weighed against the risk of hypoperfusion in ischemic tissue, even though it may reduce the elevated risk of ICH following IVT.
There is even less evidence to support aggressive blood pressure control in patients undergoing endovascular thrombectomy (EVT) for large vessel occlusion.
In the first randomized trial to specifically address blood pressure management following thrombectomy, the Blood Pressure Target in Acute Stroke to Reduce Hemorrhage After Endovascular Therapy (BP-TARGET) study compared a systolic blood pressure target of 100 to 129 mm Hg with a more permissive target of 130 to 185 mm Hg following successful reperfusion (defined as Thrombolysis in Cerebral Infarction [TICI] grade 2b or 3).
Neither improved functional outcomes nor a significant decrease in radiographic intraparenchymal hemorrhage rate at 24 to 26 hours were observed in the intensive BP-lowering group. The intensive BP-lowering group showed a nonsignificant trend toward higher mortality during the first week following EVT.
Pooled analyses and other observational studies, like Blood Pressure in Acute Stroke Evaluation (BEST), have also failed to show a definite advantage of severe blood pressure reduction following thrombectomy.
According to certain data, excessively aggressive blood pressure reduction in the context of incomplete recanalization (TICI grade <3) may worsen infarct progression and jeopardize collateral flow.
Permissive Hypertension
In stroke care, the idea of permissive hypertension has gained popularity, especially for patients who are ineligible for thrombolysis or thrombectomy.
As long as there are no other strong reasons to lower blood pressure, such as the use of IV thrombolysis therapy, successful reperfusion, myocardial infarction, aortic dissection, or hypertensive encephalopathy, current guidelines typically advise tolerating systolic blood pressure up to 220 mm Hg and diastolic blood pressure up to 120 mm Hg during the first 24 to 48 hours following a stroke.
To prevent sudden changes that could cause hypoperfusion injury, especially in people who did not receive reperfusion therapies, a cautious 15% reduction over the first 24 hours is usually advised if BP exceeds these thresholds.
Summary of Blood Pressure Control After Ischemic Stroke
1. Acute Phase Management (First 72 Hours)
For most patients with acute ischemic stroke who did not receive reperfusion therapy and have BP <220/120 mmHg, do not initiate or restart antihypertensive medications during the first 48-72 hours, as this approach does not reduce death or dependency and may be harmful. 2,4,6,7
1.1.BP Thresholds Requiring Treatment in Acute Phase
If BP ≥220/120 mmHg without reperfusion therapy: Consider cautiously lowering BP by approximately 15% over the first 24 hours, though the benefit remains uncertain.
For patients receiving IV thrombolysis (tPA): BP must be lowered to <185/110 mmHg before initiating treatment and maintained <180/105 mmHg for at least 24 hours after administration.
BP monitoring schedule after thrombolysis: every 15 minutes for the first 2 hours, then every 30 minutes for the next 6 hours, and hourly thereafter for a total of 24 hour.
For patients receiving endovascular therapy: Maintain BP <180/105 mmHg for at least 24 hours post-procedure.2
1.2.Rationale for Conservative Acute Management
Cerebral autoregulation is impaired in acute stroke, making the ischemic penumbra directly dependent on systemic BP for perfusion.
Studies demonstrate a U-shaped relationship between admission BP and outcomes, with optimal ranges between 121-200 mmHg systolic.
Rapid BP reduction can abruptly reduce perfusion to multiple organs including the brain, potentially worsening neurological outcomes.
1.3.Preferred Medications When Acute Lowering Required Labetalol is the first-line agent for acute BP control.
Nicardipine serves as an alternative, particularly in patients with bradycardia or heart failure. 8
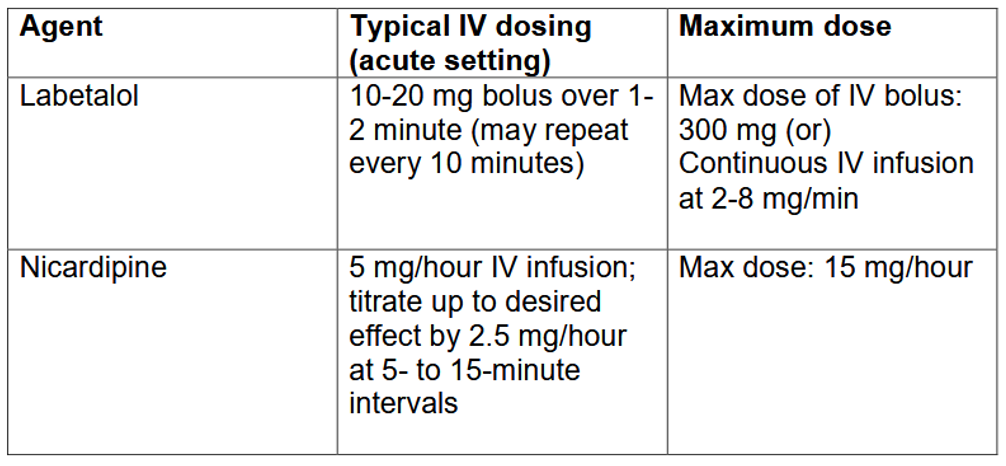
Both agents are recommended because they allow rapid titration and avoid abrupt drops in cerebral perfusion.
Avoid agents causing precipitous BP drops.
2.Subacute Phase (After 72 Hours/Day 3)
For neurologically stable patients with BP ≥140/90 mmHg who remain hypertensive after 3 days, initiate or restart antihypertensive therapy before hospital discharge.
2.1.Timing Considerations
After 3 days, the risk of cerebral hypoperfusion decreases while benefits of BP control for secondary prevention become more relevant.
Starting antihypertensive therapy during hospitalization in stable patients with BP >140/90 mmHg is safe and reasonable for improving long-term BP control.
Blood pressure lowering treatment should be initiated or modified before hospital discharge.
3.Long-Term Secondary Prevention Targets
Target BP <140/90 mmHg for general secondary stroke prevention, with consideration of <130/80 mmHg for specific patient populations.
3.1.Specific Target Recommendations
Standard target: <140/90 mmHg for most patients with prior stroke or TIA.
Lower target (<130/80 mmHg): May be reasonable for secondary prevention, particularly supported for patients with small subcortical/lacunar stroke.
Diabetic patients: Target <130/80 mmHg (systolic <130 mmHg [Evidence Level C], diastolic <80 mmHg.
Chronic kidney disease (non-diabetic): Target <140/90 mmHg.
3.2.Medication Selection
Recommended agents: Thiazide diuretic, ACE inhibitor, ARB, or combination of thiazide diuretic plus ACE inhibitor.
Selection should be individualized based on patient comorbidities and pharmacological class.
For previously treated hypertension, restart antihypertensive treatment after the first few days to reduce recurrent stroke risk.
4.Critical Pitfalls to Avoid
– Do not treat BP <220/120 mmHg in the first 48-72 hours in patients not receiving reperfusion therapy, as this has proven ineffective and potentially harmful. – Avoid excessive acute BP reduction (>70 mmHg drop) as this may cause acute renal injury and neurological deterioration.
– Do not delay restarting antihypertensives beyond 3 days in stable patients with pre-existing hypertension, as this misses the window for secondary prevention.
– Do not overlook to correct hypotension and hypovolemia to maintain systemic perfusion sufficient to support organ function, including the ischemic brain.
– Never rapidly lower BP in acute stroke, as hypotension achieved too quickly reduces perfusion to multiple organs including the brain.
5.Other Special Considerations
- Patients with severe cerebral vessel disease may benefit from a more cautious stepped-care approach targeting <140/90 mmHg rather than intensive lowering.
- More aggressive BP lowering (toward <120/80 mmHg) may benefit patients at high risk of intracranial hemorrhage.
- Patients not started on therapy in acute care require arrangements for follow-up with primary care or stroke prevention services for ongoing evaluation.
References:
- Anderson CS, Heeley E, Huang Y, et al. (2013) Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med.;368(25):2355-2365.
- Anderson CS, Huang Y, Lindley RI, et al. (2019)Intensive blood pressure reduction with intravenous thrombolysis therapy for acute ischaemic stroke (ENCHANTED): an international, randomised, open-label, blinded-endpoint, phase 3 trial. Lancet.;393 (10174):877-888.
- Chen Y, Ma Y, Qin J, et al. (2024) Blood pressure variability predicts poor outcomes in acute stroke patients without thrombolysis: a systematic review and meta-analysis. J Neurol.;271(3):1160-1169.
- De Georgia M, Bowen T, Duncan KR, Chebl AB. (2023) Blood pressure management in ischemic stroke patients undergoing mechanical thrombectomy. Neurol Res Pract.;5(1):12.
- Manning L, Hirakawa Y, Arima H, et al. (2014) Blood pressure variability and outcome after acute intracerebral haemorrhage: a post-hoc analysis of INTERACT2, a randomised controlled trial. Lancet Neurol.;13(4):364-373.
- Mazighi M, Richard S, Lapergue B, et al. (2021) Safety and efficacy of intensive blood pressure lowering after successful endovascular therapy in acute ischaemic stroke (BP-TARGET): a multicentre, open-label, randomised controlled trial. Lancet Neurol. ;20(4):265-274.
- Mistry EA, Mehta T, Mistry A, et al. (2020) Blood pressure variability and neurologic outcome after endovascular thrombectomy: a secondary analysis of the BEST study. Stroke.;51(2):511-518.
- Qureshi AI, Palesch YY, Barsan WG, et al. (2016) Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N Engl J Med.;375(11):1033-1043.
- Qureshi AI, Baskett W, Martin RH, et al. (2016) Systolic blood pressure reduction with stability as a new therapeutic goal in patients with intracerebral hemorrhage: results of the pooled analysis of ATACH 2 and INTERACT 2 trials. Neurocrit Care. Published online May 20, 2025.
Author Information
Dr. Thar Thar Oo
Senior Consultant Neurologist