Interpretation of Antinuclear Antibody (ANA) and Extractable Nuclear Antigen (ENA) Profile
Cho Mar Lwin
Introduction
The diagnosis of connective tissue diseases such as systemic lupus erythematosus (SLE), Sjögren’s syndrome, systemic sclerosis (SSc), and mixed connective tissue disease (MCTD) relies heavily on clinical symptoms, signs and baseline investigations such as full blood count indices, urine protein detection and inflammatory markers followed by identification of specific autoantibodies. Without abnormal clinical data, the positive auto antibodies are usually of no or little clinical significance.
Antinuclear antibody (ANA) screening followed by extractable nuclear antigen (ENA) profiling is the most frequently requested diagnostic cascade in suspected systemic autoimmune rheumatic diseases (SARD). While highly sensitive, the clinical utility of these tests is often compromised by improper ordering, misinterpretation of low-titre results, and failure to account for geographic and infectious confounders. In Myanmar, where infections such as tuberculosis, leprosy, and viral hepatitis can stimulate non-specific autoantibody production, a proper understanding of ANA patterns and antigen-specific ENA results is essential. A practical framework for the interpretation of ANA and ENA profiles and clinical pitfalls is of great help to practitioners.
When ordering ANA and ENA profile for a suspicious auto immune condition, the diagnostic approach follows a two-step strategy: a broad, highly sensitive initial screening test for antinuclear antibodies (ANA), followed by specific antibody testing via an extractable nuclear antigen (ENA) profile when the screen is positive.
However, because these autoantibodies can be detected in healthy individuals and during chronic infectious states, a positive test does not automatically equate to autoimmune disease. For the practicing consultant, interpreting these tests requires balancing laboratory tests against the patient’s clinical presentation.
1. Screening with ANA 2
For the interpretation of an ANA result, a clinician requires to evaluate the testing methodology, the serum titre, and the cellular staining pattern.
1.1. Methodology: The Indirect Immunofluorescence – Gold Standard 4
Indirect immunofluorescence (IIF) utilizing human epithelial (HEp-2) cells remains the international gold standard for ANA screening. HEp-2 cells are ideal because they possess large nuclei with visible mitotic structures, allowing for the expression of over 100 different autoantigens. Some laboratories still offer a latex agglutination test that reports only positive or negative result which is not as sensitive nor specific as IIF.
1.2. The Titres and Pre-Test Probability
Serum titres represent the degree to which a patient’s blood can be diluted while still showing visible fluorescence. A standard screening dilution begins at 1:40 or 1:80.
- Low Titres (1:40 to 1:80): Present in up to 30% of healthy individuals and have negligible positive predictive value. Under the 2019 EULAR/ACR classification criteria for SLE, an ANA titre of 1:80 via IIF is an obligatory entry criterion. 1
- Intermediate Titres (1:160): It could still be a significant level if it combines with relevant clinical features.
- High Titres (1:320 or 1:640 and higher): clinicians should suspect an underlying systemic autoimmune condition, necessitating further serological breakdown. However, the clinical components are major the requirements regarding the interpretation.
As the ANA positivity is highly nonspecific, it can also be found in various conditions including some organ specific auto immune diseases such as Hashimoto’s thyroiditis, coeliac disease, multiple sclerosis etc.
1.3. IIF Patterns (International Consensus on ANA Patterns – ICAP) 3
The specific visual topography of nuclear staining during IIF provides the first major clue toward the target antigen, mapping directly to distinct clinical phenotypes:
- Homogeneous: The entire nucleus is uniformly stained. This pattern reflects antibodies targeting double-stranded DNA (dsDNA) or histones, pointing strongly toward SLE or drug-induced lupus.
- Speckled: Characterized by fine or coarse graining throughout the nucleoplasm. This represents antibodies directed against the classic ENAs (Ro, La, Sm, RNP) and is seen across the spectrum of Systemic sclerosis, SLE, Sjögren’s syndrome, and MCTD.
- Centromere: Distinct, discrete dots scattered across the interphase nucleus and aligned on the metaphase plate. This pattern is highly specific for limited cutaneous systemic sclerosis (lcSSc). A few cases of Sjögren’s also have the same ANA pattern.
- Nucleolar: Staining confined to the nucleoli. This pattern is a hallmark of diffuse cutaneous systemic sclerosis (dcSSc).
- Dense Fine Speckled: A critical pattern for the general clinician to recognize. An isolated high-titre DFS70 pattern, when confirmed by antigen-specific testing, is highly prevalent in healthy individuals and effectively rules out SARD, preventing unnecessary specialist referrals and medical anxiety.
2. ENA Profile 5
When a screening ANA yields a clinically significant positive result (typically over 1:160) with a speckled or homogeneous pattern, an ENA profile should be requested. Unlike the screening ANA, an ENA profile utilizes multiplex bead assays, line immunoassays (LIA), or ELISAs to identify specific, individual autoantibodies.
The clinical associations and diagnostic utility of the some clinically useful ENA components are summarized below:
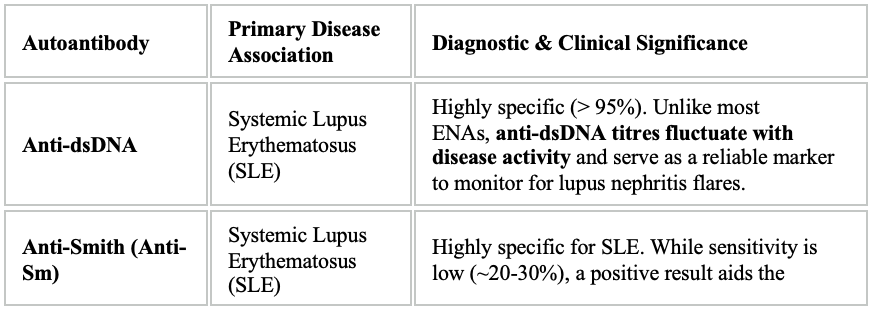
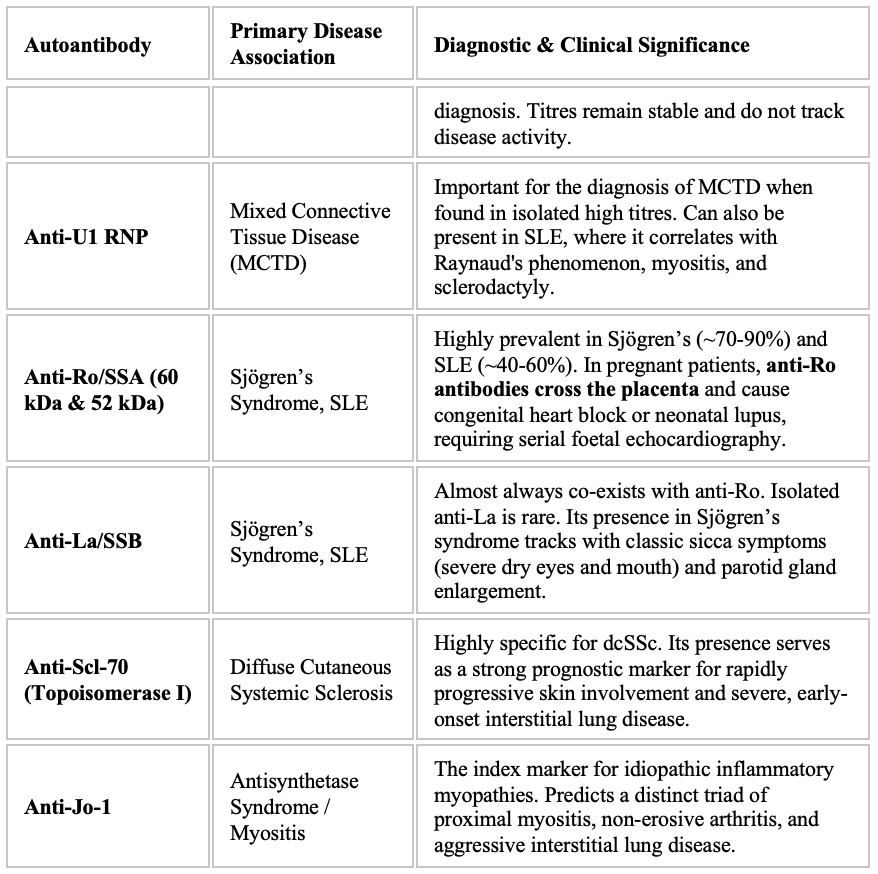
Interpretation of ENA profiles also relies on clinical data. Without clinically or biochemically suspicious auto immune condition, the positive test results of ENA profile is of no clinical relevance. Some laboratories might give additional supportive information on specific auto antibodies. These are just suggestions to help clinicians to decide. Clinicians should exercise cautious approach to reach to the diagnosis. Patients must never be labelled with a diagnosis with the specific auto antibody positivity.
3. Diagnostic Pitfalls in Daily Practice 6
3.1 Ordering “Blind” Screening Panels
The positive predictive value of an ANA test drops drastically when ordered for vague, non-specific symptoms like isolated fatigue, transient generalized arthralgia without objective synovitis, or fibromyalgia. A weak positive result in these scenarios frequently leads to patients being mislabelled with a lifelong connective tissue disease. The results of some baseline investigations such as full blood count and inflammatory markers add great value to diagnostic utility of these tests.
3.2 Repeating ANA and ENA Tests Quantitatively
A common error in clinical practice is the serial repeating of ANA or ENA profiles to check if a patient is “improving” under immunosuppressive therapy.
Clinical Rule: ANA, anti-Sm, anti-RNP, anti-Ro, and anti-La titres do not correlate with disease severity or clinical response. Once they are documented as positive, they typically remain positive for life. Repeating them incurs unnecessary healthcare expenditure. The only exceptions that warrant serial monitoring is anti-dsDNA titre in patients with SLE.
3.3 The Confounding Role of Infections
In tropical and developing healthcare settings, chronic intracellular infections represent a major diagnostic hurdle. Diseases like tuberculosis, leprosy, infective endocarditis, and chronic hepatitis B or C trigger profound, polyclonal B-cell activation. This physiological response frequently produces low-to-moderate titres of ANA and RF. Clinicians must thoroughly exclude these active infectious mimics before initiating long-term, high-dose immunosuppressive or biologic therapies.
Conclusion
The pairing of an ANA screen with a targeted ENA profile is an invaluable asset to the rheumatologist, but it must be driven strictly by clinical pre-test probability. A positive ANA is the beginning of a diagnostic investigation, not its conclusion. By understanding the methodology behind IIF, recognizing the clinical phenotypes associated with distinct ENA antigens, and keeping local infectious mimics in mind, clinicians can ensure accurate, cost-effective, and safe management of autoimmune diseases.
References
- Aringer, M., Costenbader, K., & Daikh, D. (2019). 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis & Rheumatology, 71(9), 1400–1412. https://doi.org/10.1002/art.40930
- Agmon-Levin, N., Damoiseaux, J., & Shoenfeld, Y. (2014). International recommendations for the assessment of antinuclear antibodies. Annals of the Rheumatic Diseases, 73(1), 17-23. https://doi.org/10.1136/annrheumdis-2013-203863
- Chan, E. K., Damoiseaux, J., & Carballo, O. G. (2015). Report of the first International Consensus on ANA Patterns (ICAP) 2014–2015. Frontiers in Immunology, 6, 412. https://doi.org/10.3389/fimmu.2015.00412
- Damoiseaux, J., Andrade, L. E., & Fritzler, M. J. (2019). Clinical relevance of HEp-2 indirect immunofluorescence patterns: the International Consensus on ANA Patterns (ICAP) perspective. Annals of the Rheumatic Diseases, 78(7), 879-889. https://doi.org/10.1136/annrheumdis-2018-214436
- Didier, K., Bolko, L., Giusti, D., Toquet, S., Robbins, A., Antonicelli, F., & Servettaz, A. (2018). Autoantibodies Associated With Connective Tissue Diseases: What Meaning for Clinicians? Frontiers in Immunology, 9, 541. https://doi.org/10.3389/fimmu.2018.00541
- Infantino, M., Manfredi, M., & Bizzaro, N. (2021). European League against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus: the laboratory immunologist’s point of view. Annals of the Rheumatic Diseases, 80(12), e188. https://doi.org/10.1136/annrheumdis-2019-216591
Author Information
Professor Dr Cho Mar Lwin
Professor and Head
Department of Rheumatology
University of Medicine 1 Yangon