Introduction
Plasmodium vivax infection has traditionally been regarded as a benign form of malaria compared with Plasmodium falciparum. Infection.¹ However, increasing evidence has demonstrated that P. vivax can cause severe and potentially fatal complications, even acute respiratory distress syndrome (ARDS), shock, severe anaemia, hepatic dysfunction, renal impairment, and death.²⁻⁵ We report a case of severe P. vivax malaria complicated by ARDS, septic shock, and acute hypoxemic respiratory failure requiring even invasive mechanical ventilation. This case highlights that P. vivax malaria can cause severe disease, including ARDS, septic shock, and respiratory failure requiring intensive care support. Clinicians practicing in endemic regions should recognize that vivax malaria is not always benign and may result in life-threatening complications. ², ⁵
Case Report
A previously healthy 13-year-old boy from Homalin Township, Sagaing Region, Myanmar, presented with a seven-day history of high-grade fever associated with chills and rigors. One day before admission, he developed progressive dyspnoea. On presentation, he was critically ill with septic shock and acute hypoxemic respiratory failure. Because of severe respiratory distress and refractory hypoxemia, endotracheal intubation and invasive mechanical ventilation were required. Admission chest radiography demonstrated bilateral diffuse pulmonary infiltrates consistent with ARDS. Initial laboratory investigations revealed haemoglobin 9.4 g/dL, white blood cell count 7.8 ×10⁹/L, platelet count 66 ×10⁹/L, and CRP 121 mg/L. Renal function remained normal throughout hospitalization, with serum creatinine ranging from 41–47 µmol/L. Abnormalities of liver biochemistry were noted. Malaria rapid diagnostic testing was positive for P. vivax. Peripheral blood smear microscopy demonstrated enlarged erythrocytes containing amoeboid trophozoites. Intravenous artesunate was commenced immediately according to Guideline recommended by National Malaria Control Program for severe malaria. ⁶ Empirical intravenous cefepime (1 g every 12 hours) was administered because concurrent bacterial infection could not initially be excluded. The patient showed gradual clinical improvement following treatment. Repeat malaria microscopy and rapid diagnostic testing on hospital day 3 became negative, confirming parasitological clearance. Platelet count increased from 66 ×10⁹/L on admission to 379 ×10⁹/L during recovery. Respiratory status improved steadily, permitting successful discontinuation of mechanical ventilation. Follow-up chest radiography demonstrated marked resolution of bilateral pulmonary infiltrates. After completion of intravenous artesunate therapy, ACT was given. Radical cure with primaquine (0.5 mg/kg/day) was initiated following confirmation of normal G6PD activity. The patient recovered completely and was discharged home in stable condition.
Table 1. Serial laboratory investigations during hospitalization
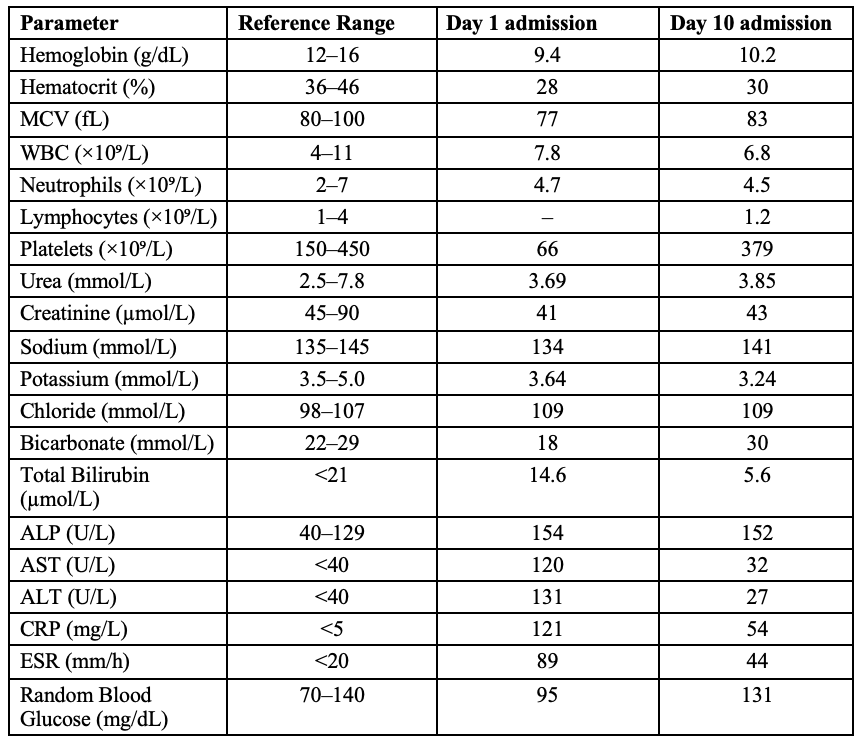

Fig. 1A-Admission chest radiograph showing bilateral diffuse alveolar infiltrates consistent with ARDS.

Fig. 1B-Follow-up chest radiograph before discharge which is completely normal.
Discussion
Historically, Plasmodium vivax was considered a relatively benign malaria species and was commonly referred to as “benign tertian malaria.”¹ Over the past two decades, however, increasing evidence has challenged this traditional view.²⁻⁵ Price and colleagues described vivax malaria as “neglected and not benign,” highlighting its capacity to cause severe anaemia, respiratory distress, multiorgan dysfunction, and death.² Subsequent systematic reviews have confirmed that severe manifestations of P. vivax include ARDS, shock, severe thrombocytopenia, acute kidney injury, hepatic dysfunction, cerebral involvement, and fatal outcomes.³⁻⁵ Professor Sir David Warrell, pioneering tropical medicine physician, also acknowledged the growing importance of severe vivax malaria and emphasized that clinicians should no longer regard P. vivax infection as invariably benign, particularly in endemic regions where severe complications are increasingly recognized.¹ This evolving understanding has important implications for clinical practice because delayed recognition of severe vivax malaria may contribute to preventable morbidity and mortality.²⁻⁵ ARDS is one of the most serious complications of severe vivax malaria.³,⁴ Several reports have documented ARDS occurring in patients with microscopically confirmed P. vivax monoinfection.³,⁴ Respiratory failure may be present at initial presentation or may develop after commencement of antimalarial therapy.³,⁴ In the present case, severe hypoxemic respiratory failure requiring mechanical ventilation was evident on admission, suggesting that pulmonary injury had already developed during the acute phase of infection. The pathogenesis of ARDS in vivax malaria remains incompletely understood. Unlike falciparum malaria, in which sequestration of parasitized erythrocytes contributes substantially to organ dysfunction, pulmonary injury in vivax malaria appears to be mediated primarily through an exaggerated inflammatory response.⁷ Increased production of pro-inflammatory cytokines may result in enhanced alveolar-capillary permeability, non-cardiogenic pulmonary oedema, diffuse alveolar damage, and impaired gas exchange.⁷ This mechanism may explain the occurrence of severe respiratory complications even in patients with relatively low parasite burdens.⁷ Our patient fulfilled WHO criteria for severe malaria because of respiratory failure requiring mechanical ventilation and the presence of shock.⁶ Thrombocytopenia was prominent at presentation, while renal function remained preserved throughout the illness. Rapid clinical recovery following intravenous artesunate, together with documented parasitological clearance, strongly supported severe P. vivax malaria as the principal diagnosis. ⁶ This case contributes to the growing body of evidence demonstrating that P. vivax is capable of causing severe malaria with life-threatening pulmonary complications. Clinicians practicing in malaria-endemic settings such as Myanmar should maintain a high index of suspicion for severe vivax malaria in patients presenting with acute febrile illness and respiratory compromise. ²⁻⁵
Conclusion
Conclusion Plasmodium vivax malaria should no longer be regarded as an invariably benign infection.² Severe manifestations including ARDS, septic shock, and acute hypoxemic respiratory failure requiring invasive mechanical ventilation may occur even in previously healthy children.³⁻⁵ Early recognition, prompt administration of intravenous artesunate, and comprehensive intensive care support are critical determinants of favorable outcomes.⁶ This case adds further evidence that P. vivax can cause severe malaria and underscores the need for continued clinical vigilance in endemic regions.
References
- Warrell DA, Molyneux ME, Beales PF. Severe and complicated malaria. Trans R Soc Trop Med Hyg. 1990;84(Suppl 2):1–65.
- Price RN, Tjitra E, Guerra CA, Yeung S, White NJ, Anstey NM. Vivax malaria: neglected and not benign. Am J Trop Med Hyg. 2007;77(6 Suppl):79–87.
- Price L, Planche T, Rayner C, Krishna S. Acute respiratory distress syndrome in Plasmodium vivax malaria: case report and review of the literature. Trans R Soc Trop Med Hyg. 2007;101(7):655–659.
- Rahman AKA, Sulaiman FN. Plasmodium vivax malaria presenting as acute respiratory distress syndrome. Trop Doct. 2013;43(2):83–85.
- Rahimi BA, Thakkinstian A, White NJ, et al. Severe vivax malaria: a systematic review and meta-analysis of clinical studies since 1900. Malar J. 2014;13:481.
- World Health Organization. Guidelines for Malaria. Geneva: World Health Organization; 2023.
- Anstey NM, Russell B, Yeo TW, Price RN. The pathophysiology of vivax malaria. Trends Parasitol. 2009;25(5):220–227.
Author Information
Aye-Mya-Theingi-Win1, Khin-Rupar-Ko2, Aye-Aye-Win3, May-Zabe4, Nyunt Thein5
- Senior Consultant physician, Tropical and Infectious Diseases Department, Yangon General Hospital
- Professor, Tropical and Infectious Diseases Department, Yangon General Hospital
- Associate Professor, Tropical and Infectious Diseases Department, University of Medicine (1), Yangon
- Senior Consultant Physician, Former Head of Department of Medicine, Emeritus Professor of Medicine, University of Medicine (1), Yangon